
Student guest post by Carrie Ellsworth
During the summer of 2010 I spent two months in Ghana studying a parasite called schistosomiasis. We worked in a small town called Adasawase to determine prevalence and treat the schoolchildren who were infected. We were told that schistosomiasis was not a major health concern for the people in the town because they were often faced with other diseases that had more immediate and severe health consequences than a parasitic infection. It became apparent that if we wanted the people of this small town to take this health threat seriously, we needed to stress the long term health sequelae that could arise due to schistosome infections.
(Personal photo taken in Ghana in 2010)
Our research group decided to implement an educational portion to our schistosomiasis control program. Through a Knowledge Attitudes and Practices survey, we found that most schoolchildren in the town reported learning about health from their teachers in school. We held a meeting with all teachers and administrators from Adasawase to educate them on the transmission, symptoms, and long term implications of schistosomiasis infections. When the possibility of greater transmission of HIV to individuals with schistosomal infections came up in discussion, we suddenly had everyone’s complete attention. You could have heard a pin drop on the cement floor of the school room.
Recently, the BBC reported that over 25% of schoolgirls between the ages of 10 and 14 in South Africa are infected with HIV. The World Health Organization has shown that HIV prevalence is much higher in females living in urban areas than in any other demographic group. More than 2/3 of the world’s population living with HIV/AIDS lives in Sub-Saharan Africa. Many efforts have been made to decrease the prevalence of HIV in Africa but few people have looked at the possibility of a parasitic infection possibly contributing to the transmission of HIV.
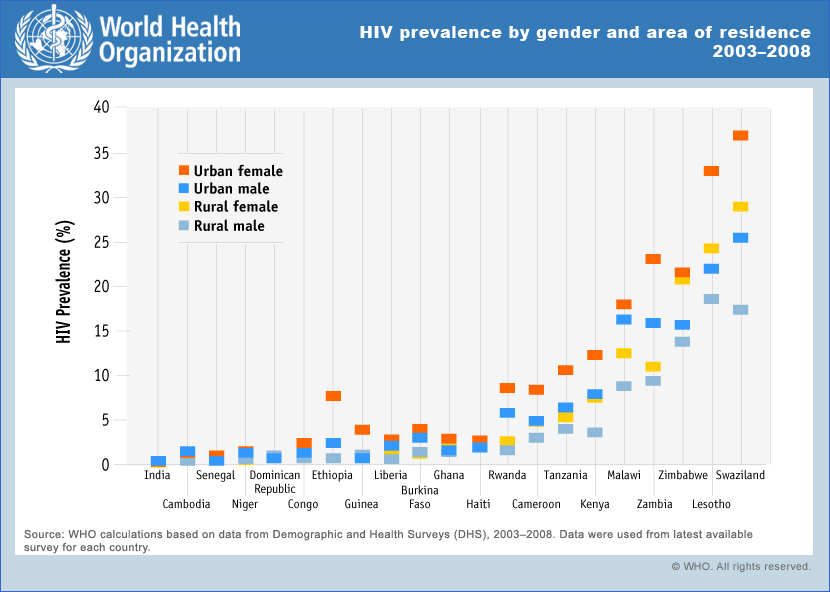
(http://www.who.int/gho/urban_health/outcomes/hiv_prevalence/en/index.ht…)
Schistosomiasis haematobium is a species of waterborne parasite that specifically affects the urogenital system of infected individuals. When people with S. haematobium urinate in stagnant water, they deposit schistosome eggs. The eggs develop into larvae which then enter a freshwater snail to continue its life cycle and mature. It leaves the snail and matures into its infective stage while in the water. The mature larval form of the parasite burrows through the skin of an individual who has contact with contaminated water. Once inside the body, the mature larva develops into an adult worm and then travels to the blood vessels surrounding the bladder. The male and female will mate to produce eggs which penetrate through the bladder wall and are passed in the urine to continue the cycle.
The treatment for a schistosomiasis infection is an inexpensive anti-helminthic medication called Praziquantel. Common signs of a S. haematobium infection are bloody and cloudy urine. Damage to the bladder wall is inevitable and if the infection becomes chronic, damage to the kidneys can also ensue. Chronic genital sores can develop in females with S. haematobium infections when the schistosome eggs are deposited in the uterus, vulva, cervix, and vagina. These lesions are believed to put the females with S. haematobium infections at a greater risk of contracting HIV. A study conducted in Zimbabwe showed that women ages 20-49, who had genital lesions due to a urogenital schistosomiasis infection, had a 3-fold higher risk of having HIV than women without a schistosomal infection.
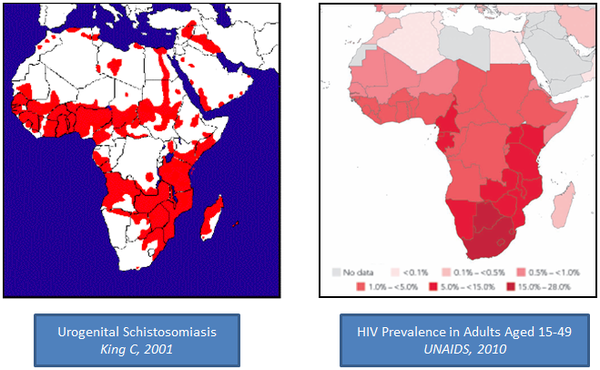
There are 207 million cases of Schistosomiasis worldwide, and 112 million of those cases are urogenital Schistosomiasis found in Sub-Saharan Africa. This creates a significant overlap between areas of Africa that are endemic to HIV/AIDS and Schistosomiasis. This has caused many scientists to question whether a greater effort to control S. haematobium infections would be an effective method of decreasing the prevalence and transmission of HIV/AIDS in Africa.
(http://blogs.plos.org/speakingofmedicine/2013/05/06/female-genital-schi…)
There is a Schistosomiasis Control Initiative (SCI) based out of London which is attempting to implement schistosome control methods in areas that are endemic. A study done in Burkina Faso showed that a single mass treatment with Praziquantel was shown to decrease the prevalence of S. haematobium by 84% in girls and 78% overall for up to 2 years. The WHO has a strategy of mass drug administration (MDA) in which school aged children in areas that have a greater than 10% prevalence of schistosomiasis would receive Praziquantel on a biannual basis, and areas that have greater than 50% prevalence would receive treatment on an annual basis. Treatment with Praziquantel results in a parasitological cure but will not heal genital lesions that have already developed from a S. haematobium infection. For this reason, prophylactic treatment starting at a young age is crucial in using this method as a means to decrease HIV prevalence.
It only costs about 32 cents to treat one child with Praziquantel. In most developing countries Praziquantel is distributed through bulk sales to the government. From there, the government dispenses its allotted Praziquantel out to different programs. The organizations that supply developing countries with Praziquantel include UNICEF and the World Health Organization among many other international organizations. Data has shown that a schistosomiasis infections increase susceptibility to HIV, elevate viral replication, exacerbate immunosuppression and increase transmission of HIV. Due to these findings, greater emphasis on schistosomiasis control is being pursued as a means of decreasing the ever growing HIV/AIDS prevalence in Africa. Widespread distribution of Praziquantel to schoolchildren in countries endemic to both schistosomiasis and HIV/AIDS could potentially prevent 120,000 new cases of HIV/AIDS in the next decade.
If treatment with Praziquantel for one child costs $0.32, then treating 70 million children would cost $22 million for one year. If a 10 year plan was implemented that treated every one of those 70 million children biannually, that would cost approximately $112 million. Compare that with the $18.8 billion that has been proposed to be spent over the next 5 years by the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR). The cost of treating 70 million children for schistosomiasis over a 10 year span is dwarfed by the projected costs of the PEPFAR and could potentially make a significant change in the rising trend of HIV infections in Africa.
All of the research points towards mass treatment with Praziquantel as being the most cost effective and successful method of decreasing the number of schistosomiasis infections and HIV/AIDS transmission. The cooperation between HIV and schistosomiasis control programs is critical in ensuring the success of such a program. Combatting two of Africa’s top health concerns with one simple low cost medication would do wonders for lowering the morbidity and mortality rates of many African countries.
References:
"HIV and AIDS Statistics: Worldwide." Statistics: Worldwide. AmfAR, Nov. 2012. Web. 10 June 2013. <http://www.amfar.org/about_hiv_and_aids/facts_and_stats/statistics__wor…;.
Hotez PJ, Fenwick A (2009) Schistosomiasis in Africa: An Emerging Tragedy in Our New Global Health Decade. PLoS Negl Trop Dis 3(9): e485. doi:10.1371/journal.pntd.0000485
Hotez, Peter J., Alan Fenwick, and Eyrun F. Kjetland. "Africa's 32 Cents Solution for HIV/AIDS." PLoS Neglected Tropical Diseases 3.5 (2009): E430. Print.
"International Strategies for Tropical Disease Treatments - Experiences with Praziquantel - EDM Research Series No. 026: Chapter 5: The International Supply of Praziquantel*: Global Distribution of Praziquantel."
International Strategies for Tropical Disease Treatments - Experiences with Praziquantel - EDM Research Series No. 026: Chapter 5: The International Supply of Praziquantel*: Global Distribution of Praziquantel. World Health Organization, 2013. Web. 10 June 2013.
Kosinski, Karen C., Kwabena M. Bosompem, Miguel J. Stadecker, Anjuli D. Wagner, Jeanine Plummer, John L. Durant, and David M. Gute. "Diagnostic Accuracy of Urine Filtration and Dipstick Tests for Schistosoma Haematobium Infection in a Lightly Infected Population of Ghanaian Schoolchildren." Acta Tropica 118.2 (2011): 123-27. Print.
"Schistosomiasis." World Health Organization. Web. 10 June 2013. <http://www.who.int/mediacentre/factsheets/fs115/en/>.
"Schistosomiasis: Epidemiological Situation." World Health Organization. N.p., n.d. Web. 10 June 2013. <http://www.who.int/schistosomiasis/epidemiology/en/>.
Secor, Evan W. "The Effects of Schistosomiasis on HIV/AIDS Infection, Progression, and Transmission." Current Opinions on HIV and AIDS 7.3 (2012): 254-59. Print.
Simon, Gregory. "Combined Schistosomiasis and HIV Control Programs: Saving Lives AND Money”. End the Neglect. N.p., 7 May 2013. Web. 11 June 2013. <http://endtheneglect.org/2013/05/combined-schistosomiasis-and-hiv-contr…;.
"South Africa: 'Over 25% of Schoolgirls HIV Positive'" BBC News. BBC, 14 Mar. 2013. Web. 10 June 2013. <http://www.bbc.co.uk/news/world-africa-21783076>.
Temple, Bliss. Schistosoma Haematobium (blood Flukes). Schistosomiasis Haematobium (blood Flukes). Stanford University, May 2004. Web. 10 June 2013. <http://www.stanford.edu/class/humbio103/ParaSites2004/Schisto/website.h…;.