
It's no secret that I'm not particularly fond of the National Center for Complementary and Integrative Health (NCCIH). Formerly known as the National Center for Complementary and Alternative Medicine (NCCAM) and before that the Office of Alternative Medicine, NCCIH has been the foremost government agency funding research into quackery and the "integration" of quackery into medicine for the last 24 years, which is, of course, the reason I've been been harshly critical of NCCIH since very early in the history of Respectful Insolence. Basically, NCCIH not only funds studies of dubious "alternative" therapies, but it also promotes quackery by funding "fellowships" at various institutions to teach "integrative medicine," or, as I like to call it, "integrating" quackery with real medicine. There's a reason why I say we take off and nuke the entire center from orbit. It’s the only way to be sure.
Indeed, back in 2009, when President Barack Obama first took office, Steve Novella and I both suggested that the time was ripe for NCCIH to be defunded and its functions allowed to revert back to the already existing Institutes and Centers of the National Institutes of Health. We were under no illusions that this would happen, given that NCCIH always had a powerful protector in the man who was arguably more responsible for creating NCCIH and guarding it against all attempts at defunding or, even worse, forcing it to do more rigorous science, woo-loving Senator Tom Harkin (D-IA). Harkin is no longer in the Senate, having retired at the end of 2014, but NCCIH is still with us, and the nature of government makes it very much that, unless someone with power is willing to expend serious political capital to eliminate it, NCCIH will be with us always, no matter how much it tries to change its name to eliminate anything implying pseudoscience.
So those of us who recognize that NCCIH was created to promote the "integration" of "outside of the mainstream" or "unconventional" treatments (the vast majority of which are quackery) into real medicine have to learn to live with NCCIH and, as much as it might gall us, to try make lemonade out of the lemon by prodding it to doing some actual rigorous science on "complementary and alternative medicine" that have at least a modicum of biological plausibility and avoid wasting taxpayer money on fairy dust treatments whose precepts either violate the laws of physics (e.g., reiki, homeopathy, and other "energy" medicine) or depend on nonexistent anatomy or physiology (e.g., reflexology, craniosacral, traditional Chinese medicine tongue diagnosis).
This brings me to something I saw on the NCCIH Director's Blog a week and a half ago, a post by the director Josephine Briggs, Requesting Comments on NCCIH's Draft Strategic Plan. Patriotic US citizen and advocate of SBM that I am, how could I turn down such a request? Kimball Atwood didn't shirk from such a request back when Dr. Briggs was asking for comments on the NCCAM 2011-2015 strategic plan, nor did I. This time around, I'm half tempted to say: Meet the old plan, same as the old plan (almost).
The NCCIH 2016-2021 draft strategic plan: Overview
I plan on discussing each objective in the plan, but before I do it's useful to get the "bird's eye" view and compare it to previous NCCIH plans. As I read through the draft of the NCCIH 2016-2021 strategic plan, I couldn't help but feel a profound sense of déjà vu. In fact, much of the new strategic plan draft sounds suspiciously similar to the old plan. Let's take a look at the goals and objectives of the old strategic plan first:
- GOAL 1: Advance the science and practice of symptom management.
- GOAL 2: Develop effective, practical, personalized strategies for promoting health and well-being.
- GOAL 3: Enable better evidence-based decision making regarding CAM use and its integration into health care and health promotion.
And the strategic objectives to be used to accomplish these goals:
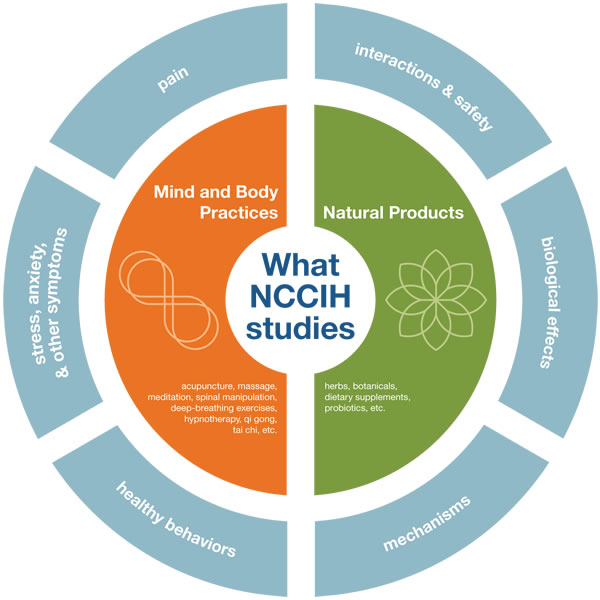
- Strategic Objective 1: Advance Research on Mind and Body Interventions, Practices, and Disciplines
- Strategic Objective 2: Advance Research on CAM Natural Products
- Strategic Objective 3: Increase Understanding of "Real-World" Patterns and Outcomes of CAM Use and Its Integration Into Health Care and Health Promotion
- Strategic Objective 4: Improve the Capacity of the Field To Carry Out Rigorous Research
- Strategic Objective 5: Develop and Disseminate Objective, Evidence-Based Information on CAM Interventions
Now, let's compare to the new plan, which has eliminated overarching goals and simply lists five strategic objectives:
- Objective 1: Advance Fundamental Science and Methods Development
- Objective 2: Improve Care for Hard-to-Manage Symptoms
- Objective 3: Foster Health Promotion and Disease Prevention
- Objective 4: Enhance the Complementary and Integrative Health Research Workforce (cross-cutting)
- Objective 5: Disseminate Objective Evidence-based Information on Complementary and Integrative Health Interventions (cross-cutting)
In the place of overarching goals, the draft 2016-2021 plan now lists several scientific priorities, stating that this part of the plan will be a "living" document, to be "updated based on public health needs, new scientific opportunities, research results, changes in the Center's grant portfolio, and budgetary considerations":
- Nonpharmacologic Management of Pain
- Neurobiological Effects and Mechanisms
- Innovative Approaches for Establishing Biological Signatures of Natural Products
- Disease Prevention and Health Promotion Across the Lifespan
- Clinical Trials Utilizing Innovative Study Designs to Assess Complementary Health Approaches and Their Integration into Health Care
- Communications Strategies and Tools to Enhance Scientific Literacy and Understanding of Clinical Research
One can't help but notice the similarity between the two plans, at least in outline. For instance, Objectives 1 and 4 in the new plan are little more than a repackaging of Objective 4 in the old plan, all of which carry with them an implicit admission of how poor the science carried out by NCCIH-funded investigators has been over the years. Indeed, one of the sub-objectives of Objective 1 is to "Develop new and improved research methods and tools for conducting rigorous studies of complementary health approaches and their integration into health care." Objective 5 is even more similar in both plans; the two even have almost identical wording. Meanwhile, Objective 3 in the old plan is basically the same as one of the scientific priorities, namely "Clinical Trials Utilizing Innovative Study Designs to Assess Complementary Health Approaches and Their Integration into Health Care." Of course, whenever you see any sort of discussion of "innovative study design" with respect to CAM modalities, it almost always means "coming up with study designs that make it look as though this quackery actually works."
Of course, there is nothing fundamentally wrong with a new five year plan strongly resembling the previous five-year plan. When a new five year plan so strongly resembles the five year plan immediately preceding it, however, it's hard not to wonder what progress has been made on the objectives shared by both plans and whether something new needs to be done to meet those objectives. For instance, as I said about the last plan, arguing for applying more rigorous science to just about anything is rather like arguing for mom, apple pie, and the flag; no one is going to contest that as a worthy goal. The problem, of course, is what one means by "rigorous science" and how one proposes to achieve that goal.
So let's look at the objectives, but we should do so in the context of the stated mission of NCCIH, which is reiterated in the plan's introduction:
The mission of NCCIH is to define, through rigorous scientific investigation, the usefulness and safety of complementary and integrative health interventions and their roles in improving health and health care.
And:
To address the need for objective evidence as to the safety and efficacy of many of these approaches, NCCIH supports rigorous scientific investigation to better understand how these interventions work, for whom, and the optimal methods of practice and delivery.
One can't help but note the language. It's not "if" these interventions work, but "how," "for whom," and the "optimal methods of practice and delivery," all of which are putting the cart before the horse. The introduction also repeats the standard tropes about one-third or more of adult Americans using some form of CAM, in which exercise like yoga, dietary interventions, and vitamin supplements are counted as being "CAM." I refer to this as a "trope," because there is nothing alternative about any of this; it is simply a "rebranding" of what should be part of SBM as somehow being "alternative" when it is not, a "rebranding" that is reemphasized later in the introduction:
NCCIH also seeks to identify strategies for promoting health and preventing disease. Behavioral risk factors, including an unhealthy diet, being overweight or obese, living a sedentary life, smoking or using tobacco products, and the excessive consumption of alcohol, are linked to increased rates of cardiovascular disease, cancer, and diabetes. Preliminary evidence indicates that some complementary health approaches may be useful in encouraging improved self-care, an improved personal sense of well-being, and a greater commitment to a healthy lifestyle. For example, analysis of the 2012 NHIS data indicates that many people who practiced yoga reported that it motivated them to practice healthier behaviors, including eating better and exercising more regularly. While causal relationships between the practice of complementary approaches and healthy behaviors have not been established, further research is needed to explore, clarify, and examine their relationship.
Once again, there is nothing "alternative" or "integrative" about any of this. Any primary care doctor worth his or her salt will counsel patients to eat healthier, lose weight, stop smoking, decrease alcohol intake, and get off their butts and exercise. I hear the part about losing weight, eating better, and exercising every time I see my doctor. (Fortunately, I don't smoke and don't overindulge in alcohol.) As for yoga, is there anything better about it that motivates people to practice healthier behaviors, beyond what any sort of exercise would accomplish? Again, none of this is in any way "alternative" or "integrative," and none of it needs a special center at the NIH to study it.
It is also important to note that NCCIH is now emphasizing, as its key scientific priority, pain and difficult-to-control symptoms, in particular nonpharmacologic methods of relieving pain. While there is certainly a need for better research into how better to control pain without non-steroidal anti-inflammatory drugs or opioids, both of which have significant side effects and the latter of which is recognized as a significant cause of addiction and premature death, one can't help but note that these are also problems where assessing the benefit of any therapy is very much compounded by placebo effects, regression to the mean, and the like. Yet, elsewhere in the plan, NCCIH addresses how to do "innovative clinical trials" by using "pragmatic clinical trials to address questions about the integration of complementary health approaches into health care systems, or to study the effectiveness of complementary or integrative approaches in comparison to standard care." Remember, pragmatic trials are trials that are done only after more rigorous trials actually show that an intervention works, with the intent to see how it works in the "real world." Doing pragmatic trials of treatments not yet shown to work is putting the cart before the horse.
On the other hand, it's good to know that NCCIH has finally accepted that plausibility is important:
As a responsible steward of its publicly provided resources, NCCIH is highly selective in the choice of topics for major clinical trials. Decisions about which large-scale trials to support must be based on the strength, reliability, and reproducibility of signals from clinical experience and preliminary, smaller pilot studies, as well as on evidence of scientific plausibility obtained from mechanistic studies.
Of course, there appears to be a bit of a problem in defining what "plausibility means." Now, it is true that NCCIH hasn't funded a study of homeopathy since 2008, as I have pointed out before, and the lack of further funding of homeopathy argues that NCCIH leadership might really mean it about scientific plausibility. On the other hand, given how enamored NCCIH remains with modalities like acupuncture and various modalities from traditional Chinese medicine (TCM) that are rooted in a prescientific understanding of physiology and disease, I can't help but say to NCCIH: Plausibility. You keep using that word. I do not think it means what you think it means.
Now let's look at the objectives.
Objective 1: Advance Fundamental Science and Methods Development
As I said before, this objective is pretty much the "mom and apple pie" objective in that no one is going to argue against improving fundamental science and methods. The major problem with this objective is that it is so generic. It is an objective that pretty much any institute or center at the NIH would have. One of the key complaints we have about NCCIH is that it doesn't serve a purpose that couldn't be just as well served elsewhere in the NIH and that there is really no scientific justification for separating CAM from the rest of medicine, later to "integrate" it, or for needing a separate specialty. There's an oft-stated aphorism in skepticism that there is no such thing as alternative medicine. There is medicine that has been scientifically demonstrated to be safe and effective; there is medicine that has not been scientifically demonstrated to be safe and effective; and there is medicine that has been scientifically demonstrated to be ineffective or even harmful. Most alternative medicine falls into the latter two categories. Moreover, when any "alternative" or "outside the mainstream" treatment is demonstrated to be safe and effective through science, it ceases to be "alternative" and becomes just "medicine."
On the other hand, I would rather see NCCIH devote resources to this objective for the simple reason that the advances that result would be applicable not just to the study of "alternative" health practices but to medicine in general. After all, when NCCIH lists as a strategy in this objective, "Advance understanding of basic biological mechanisms of action of natural products, including probiotics," I point out that this is nothing more than natural products pharmacology of the type that has been done for decades in academia and industry, where active compounds are purified and isolated from natural sources. Similarly, the studies in this objective designed to "confirm the link between the impact of the natural product on a biological signature (i.e., mechanism of action) and demonstrate an association between the change in the biological signature and clinical outcomes in humans" are nothing but more of the same. Again, none of this is anything different than what is done for drug and device development elsewhere; so, if NCCIH must exist, it would do the least harm and the most good using its resources for these ends, my distaste for the "rebranding" of natural products pharmacology and drug development as somehow "integrative" notwithstanding. The more resources NCCIH devotes to Objective 1, the less it has for pseudoscience.
Objective 2: Improve Care for Hard-to-Manage Symptoms
There is no doubt that there are a number of conditions and symptoms that conventional medicine has a hard time dealing with. Chronic pain is, of course, one of the most common and worst. It is also a major source of morbidity and mortality due to opioid addiction, often with an iatrogenic origin beginning with a prescription for opioid pain relievers. Consequently, it is certainly important to improve care for chronic pain and other difficult-to-manage symptoms. The problem with this objective is that it is not at all clear how the proposed methodology will lead to improved care for patients suffering from such hard-to manage symptoms. For instance, NCCIH proposes studying the use of natural products and probiotics for symptom management to "confirm the link between the impact of the natural product on a biological signature (i.e., mechanism of action) and demonstrate an association between the change in the biological signature and clinical outcomes in humans." Yet there is little evidence to support this approach over any other pharmacologic approach. The same is true of so-called mind-body practices, an area that NCCIH places a great deal of its stock in.
Let's recap what NCCIH means by "mind and body" approaches. I'll take its definition from its last strategic plan, given that no new definition is proposed in the current draft plan. The definition is so vague as to be essentially meaningless, as NCCIH describes "mind and body" or "mind-body" interventions as:
These interventions, practices, and disciplines are grouped together in this plan as mind and body* approaches because, from a research perspective, they all share a set of characteristics that create similar challenges in designing rigorous and definitive clinical investigations of their benefit and safety. For example, (1) it is generally difficult or impossible to mask practitioners and/or participants involved in clinical research, (2) claims about benefit often relate to subjective clinical outcomes, (3) in practice, the interventions are often individualized, or they are complicated procedures that are difficult to systematize or characterize fully, and (4) means to objectively measure the impact of the interventions on important biological processes are frequently lacking, particularly those that purport to act through processes not understood or well characterized by modern science.
*Terminology: As used in this plan, mind and body encompasses interventions from the three domains of mind/body medicine, manipulative and body-based practices, and energy medicine.
Examples listed included:
- Acupuncture
- Breath practices
- Meditation
- Guided imagery
- Progressive relaxation
- Tai chi
- Yoga
- Spinal manipulation
- Massage therapy
- Feldenkrais method
- Alexander technique
- Pilates
- Hypnosis
- Trager psychophysical integration
- Reiki
- Healing touch
- Qi gong
- Craniosacral therapy
- Reflexology
Notice that there's a whole lot of quackery in there (e.g., reiki, healing touch, craniosacral therapy, acupuncture, reflexology) mixed in with the potentially useful, such as guided imagery, progressive relaxation, and meditation. That's why, right off the bat, I'm not sure if what is meant by "mind and body" interventions in the 2016-2021 strategic plan draft is the same as what NCCIH meant in its 2011-2015 plan, because in the most recent draft plan, it describes "mind and body" interventions as "massage, acupuncture, yoga, and meditation, and natural products, such as herbs, fish oil, melatonin, and probiotics." The definition is as amorphous as the definition of CAM, and it appears to change to mean whatever NCCIH needs it to mean, such that one can't help but think of Humpty Dumpty's famous statement, "When I use a word, it means just what I choose it to mean—neither more nor less."
"Fluidity" of language or not, it's a good thing that the quackery appears to be gone. Indeed, on the NCCIH web page on Mind and Body Practices, the only blatant quackery left is acupuncture, with the rest including massage therapy, meditation, relaxation techniques, spinal manipulation, and yoga. However, it is odd that NCCIH did not explain why it changed its definition. Whatever the reason for the change, many of these "mind and body" interventions, other than acupuncture, are nothing that needs a separate "alternative" label or that requires a separate center to study them. If they were going to be studied with rigorous science, then, again, my distaste for the "rebranding" going on here notwithstanding, it would be a good thing that NCCIH is using its resources this way rather than to study homeopathy or "energy medicine."
On the other hand, NCCIH giveth, and NCCIH taketh away. While saying it's going to use rigorous science to study mind and body interventions, it then concludes this objective thusly:
Given the widespread use of complementary health approaches, opportunities exist to employ clinical outcomes and effectiveness research methodologies to collect "real world" evidence about the use of specific complementary approaches for health care and health promotion. Pursuing this type of research requires creative collaboration with those who provide care in settings where integration of complementary health approaches could be studied. The "real-world" settings for such research may be quite varied, and could include schools, nursing homes, hospices, cancer treatment facilities, and settings that provide care for military personnel and Veterans.
This is simply another mention of "pragmatic" studies, or putting the cart before the horse. Again, pragmatic studies are useful for seeing how treatments that have already passed muster in randomized controlled trials (RCTs) perform in "real life," but they cannot themselves demonstrate efficacy unless the effect size is so enormous as to be undeniable, something that is seldom seen in clinical research and virtually never seen in CAM research. Basically, one purpose of pragmatic studies in CAM research is to serve as an excuse to substitute lower quality, less rigorous clinical investigation evidence showing that a CAM intervention "works" for the more rigorous RCT evidence that failed to find an effect. NCCIH really needs to remove or greatly deemphasize this reliance on pragmatic studies to investigate CAM interventions if it wants to be taken seriously by scientists. Of course, if NCCIH did that, it would have almost nothing left in terms of clinical investigation.
 The CAM in "integrative medicine" is rather like adding Chocolate Frosted Sugar Bombs as "part of a healthy breakfast."
The CAM in "integrative medicine" is rather like adding Chocolate Frosted Sugar Bombs as "part of a healthy breakfast."
There is another purpose of "pragmatic" research as well. As Steve Novella has described, pragmatic studies of CAM are in essence a bait-and-switch, which he likens to the "part of this nutritious breakfast" con, in which something like Chocolate Frosted Sugar Bombs is described as "part" of such a breakfast because the rest of the breakfast is nutritious all by itself; so it's still nutritious even with the Sugar Bombs. It's the same way CAM researchers add something like acupuncture to another intervention, even though they can't separate out the variables, and conclude that acupuncture (or insert your favorite CAM treatment here) is part of a "healthy regimen," even though it is irrelevant.
Which, appropriately enough, brings us to Objective 3. Remember Chocolate Frosted Sugar Bombs when reading this next section.
Objective 3: Foster Health Promotion and Disease Prevention
Objective 3 is perfect example of what Steve was talking about. It's basically studying the addition of Chocolate Frosted Sugar Bombs as part of a healthy breakfast. In other words, it's the "integration" of interventions that are "alternative" by virtue of being science-based modalities rebranded as alternative or integrative (like exercise and nutrition) or are quackery (like acupuncture), the implication being that they are necessary or very helpful to a "health-promoting" lifestyle. Some interventions (the rebranded ones) might actually be part of that healthy breakfast. Other interventions (like acupuncture) are Chocolate Frosted Sugar Bombs.
Moreover, the vast majority of Objective 3 consists of yet more examples of putting the cart before the horse; i.e., studying how to add the Chocolate Frosted Sugar Bombs to the breakfast without first determining whether they should be added in the first place. This objective proposes three strategies to achieve its end:
- Investigate mechanisms of action of complementary and integrative health approaches in health resilience and practices that improve health and prevent disease.
- Study complementary health approaches to promote health and wellness across the lifespan in diverse populations.
- Explore research opportunities to study and assess the safety and efficacy of complementary health approaches in non-clinical settings such as community- and employer-based wellness programs.
One notes a heavy emphasis on using pragmatic studies of how CAM "works" in the "real world" and a distinct lack of emphasis on studying whether CAM "works" in the first place. I would counter that Objective 3 is premature and that NCCIH, if it must exist, should study whether CAM has beneficial health effects, not how to integrate CAM with medicine. Of course, NCCIH is not likely to do this because its stakeholders, particularly the ones with representation on the National Advisory Council for Complementary and Integrative Health (NACCIH), the advisory council to which Dr. Briggs answers, do not want it, given how many naturopaths, acupuncturists, and chiropractors sit on the council. Remember, NCCIH was originally created as a mechanism to legitimize alternative medicine, which is why Sen. Harkin so famously expressed disappointment several years ago that NCCIH wasn't validating enough quackery.
Objective 4: Enhance the Complementary and Integrative Health Research Workforce
Here's another objective that is like arguing for mom and apple pie. Who can argue against improving the research workforce? I can, at least if that workforce is being trained to study treatments that likely have no value, particularly considering these aims in the objective:
In particular, the Center will focus on:
- Clinician-scientists, including conventionally trained physicians, complementary health practitioners, and other health care professionals (e.g., clinical psychologists, nurses) who conduct research across a wide range of complementary and integrative heath approaches.
- Scientists trained in key biomedical and behavioral research disciplines necessary for rigorous, state-of-the-art scientific investigation of complementary and integrative health interventions, practices, and disciplines.
- Individuals from groups who are underrepresented in scientific research (e.g., racial and ethnic minority populations) and are interested in careers in complementary and integrative health research.
For one thing, if these researchers are trained, who will fund them, given the prolonged budget crunch at NIH that began over a decade ago and has led to periods of record low grant funding rates? Even the NCCIH budget has been flat. More importantly, I would argue that these clinician-scientists and scientists would be far better utilized studying more promising interventions than anything NCCIH currently funds. Remember, what NCCIH is talking about here is training grants, and NCCIH training grants have not had a good record of promoting evidence- and science-based knowledge and skills about medicine. Still, if NCCIH must exist, training scientists in research methodology would be less harmful than wasting money studying and promoting homeopathy or "energy medicine."
Next up...
Objective 5: Disseminate Objective Evidence-based Information on Complementary and Integrative Health Interventions
This is yet another "mom and apple pie" objective. The main problem with it is what NCCIH might promote, as its definition of "evidence-based information" does not necessarily jibe with what really is evidence-based information. In fact, I actually hope that NCCIH really does promote objective, evidence-based information on CAM, that it really is serious about it. If so, it would tell people that homeopathy is nothing but water, that there is no evidence that reiki practitioners can manipulate a "universal energy field" to heal, and that there's no scientifically convincing evidence that practitioners of therapeutic touch can detect or manipulate human energy fields. Let's look at what NCCIH says about reiki, because reiki is as pure a quackery as homeopathy:
Reiki is based on an Eastern belief in an energy that supports the body's innate or natural healing abilities. However, there isn't any scientific evidence that such an energy exists.
OK, close, but not quite. Reiki does depend on a belief in "energy" that practitioners can supposedly channel into patients for healing effect. NCCIH doesn't mention that that "energy" comes from something called the "universal source." When you look at it that way, what reiki very much resembles faith healing, substituting Eastern mystical beliefs for Judeo-Christian beliefs. If you don't believe me, just substitute "God" for "universal source."
Then it goes wrong:
Several groups of experts have evaluated the evidence on Reiki, and all of them have concluded that it's uncertain whether Reiki is helpful.
Only a small number of studies of Reiki have been completed, and most of them included only a few people. Different studies looked at different health conditions making it hard to compare their results. Many of the studies didn't compare Reiki with both sham (simulated) Reiki and with no treatment. Studies that include both of these comparisons are usually the most informative.
No, when there is no evidence that reiki "energy" exists and the intervention has as low a scientific plausibility as reiki, it's safe to say that it doesn't work.
Here's what NCCIH says about homeopathy:
There is little evidence to support homeopathy as an effective treatment for any specific condition.
More like no convincing evidence, but I won't quibble about that. Also:
Homeopathy is a controversial topic in complementary health research. A number of the key concepts of homeopathy are not consistent with fundamental concepts of chemistry and physics. For example, it is not possible to explain in scientific terms how a remedy containing little or no active ingredient can have any effect. This, in turn, creates major challenges to rigorous clinical investigation of homeopathic remedies. For example, one cannot confirm that an extremely dilute remedy contains what is listed on the label, or develop objective measures that show effects of extremely dilute remedies in the human body.
What a weaselly, wishy-washy way of describing homeopathy. No, homeopathy is not controversial scientifically. Its precepts violate fundamental concepts in chemistry and physics. Barring a major change in the understanding of those precepts, by what we know about physics and biochemistry now, homeopathy cannot work. That is the main "challenge" to doing clinical trials of homeopathy and the main reason why such trials are not scientifically fruitful or even ethical. Even considering only clinical evidence, taken as a whole, clinical trials are consistent with homeopathy having no effect over that of placebo. Clearly NCCIH has a way to go to improve its objective, evidence-based assessments.
Finally...
Top Scientific Priorities
NCCIH proposes these as its current top scientific priorities:
- Nonpharmacologic Management of Pain
- Neurobiological Effects and Mechanisms
- Innovative Approaches for Establishing Biological Signatures of Natural Products
- Disease Prevention and Health Promotion Across the Lifespan
- Clinical Trials Utilizing Innovative Study Designs To Assess Complementary Health Approaches and Their Integration Into Health Care
- Communications Strategies and Tools To Enhance Scientific Literacy and Understanding of Clinical Research
I've already touched on some of these areas above; so I won't go into too much detail. I can't help but note that many of the research priorities here again assume that much of CAM works and that there are, for instance, biomarkers that will correlate with various CAM interventions having a biological effect, not asking if these CAM interventions actually have a therapeutic effect. Once again, we see a proposal to conduct "large, pragmatic studies of pain management addressing important clinical or health systems questions." Such studies would be virtually guaranteed to be positive and "validate" almost any CAM intervention you can think of; pragmatic studies of CAM should not be done absent compelling RCT results showing efficacy.
One interesting thing I couldn't help but notice were areas the NCCIH calls "Areas of Low Programmatic Priority." First, I noticed these:
- Research comparing clinical outcomes of verum and sham acupuncture.
- Research comparing individualized to standardized acupuncture treatment protocols.
The naïve one in me would like to think that these areas were given low priority because the questions have been answered resoundingly. We know that there is no difference between "real" and "sham" acupuncture in results, and we know that individualizing acupuncture treatments makes no difference. As I like to say, it doesn't matter where you stick the needles or even if you stick the needles in.
There was also another set of interesting areas of low priority, this time in natural products:
- Research focused on a single compound or well-characterized mechanistic target.
- Screening of natural product libraries in subcellular assays.
- Bioactivity-guided fractionation projects.
These are basically standard pharmacological studies. You look at one drug and one cellular target for that drug. Or you can screen libraries of natural products for activity using various biochemical assays. Or you fractionate a crude plant extract looking for the fractions that have activity. In other words, NCCIH has relegated to "low programmatic priority" anything resembling standard pharmacology in favor of looking for biological "signatures" due to crude extracts for which the active compounds might be many, looking for that mystical "synergy." In other words, NCCIH is assuming without evidence that "natural" crude extracts are better than single compounds.
Finally, I couldn't help but laugh at these last three low priority areas:
- Large-scale clinical trials of mind and body interventions when there are no preliminary data to determine appropriate dose, duration, and frequency or whether the patient population can adhere to the proposed intervention.
- Large-scale clinical trials of natural products when there are no preliminary data demonstrating the availability, bioavailability, and pharmacokinetics of the product; a replicable effect on a biologic signature; and dosing studies to determine the appropriate dose to impact the biologic signature.
- Pragmatic trials of interventions that do not have preliminary data demonstrating clinical efficacy or effectiveness in large controlled trials.
Did you see that last one? NCCIH says throughout this strategic plan that it wants to do more "pragmatic" trials, and here it says that such trials are of low priority if there are not preliminary data from large RCTs demonstrating efficacy. That's quite a conundrum NCCIH has created for itself there, particularly when it says in the previous two low-priority items that it won't do large-scale clinical trials of CAM or natural products without good preliminary data or a replicable effect on a biological signature. I can't help but note that if NCCIH really did adhere to these guidelines, it would never fund any clinical trials at all. Of course we all know that NCCIH will fund clinical trials, because its stakeholders won't long stand for this much rigor. It'll find ways to justify them and appear as though it's not ignoring its strategic plan.
Don't get me wrong. As I've said before, NCCIH has improved under Dr. Briggs' stewardship. She has, for the most part, eliminated funding for the worst quackery, such as homeopathy, although when Steve Novella, Kimball Atwood, and I met with her six years ago she wouldn't—or couldn't—say that NCCIH would not fund homeopathy studies any more, and in retrospect seemed to be meeting with us and homeopaths in order to be able to say she had "listened to both sides" more than anything else. Unfortunately, NCCIH still remains enamored of acupuncture and some "energy medicine," such as healing touch.
Like integrative medicine, NCCIH has evolved. Its original purpose was to validate a lot of alternative medicine because a woo-friendly senator wasn't happy with the way that the NIH concerned itself with little things like scientific plausibility and rigorous scientific evidence in evaluating health interventions. In the beginning, it wasn't that sophisticated about it and tested all sorts of wild alternative medicine, such as homeopathy, distant healing, and the like. As criticism mounted and the evidence became clearer and clearer that that woo didn't work, eventually NCCIH started concentrating on areas less obviously pseudoscientific and, of course, on rebranding conventional science-based interventions like diet and exercise as somehow being part of CAM or "integrative medicine". It had to.
The NCCIH 2016-2021 draft strategic plan is evidence of just how narrow NCCIH's purview has become. Over the last 20 years, it's failed to validate a single alternative medicine intervention, and, one by one, the more quacky ones have become unsupportable, even by NCCIH. All that's left now are rebranded SBM interventions. As I like to say, integrative treatments that might have a basis in science tend, from a scientific perspective, to be pretty mundane. In the world of "integrative medicine," all the "sexy" interventions are the ones based in myth, prescientific ideas, and pseudoscience, like homeopathy, acupuncture, and TCM, and it's all of those that NCCIH has largely—but not completely—been forced to abandon.
The problem at the heart of this strategic plan is that, minus the study and promotion of quackery, NCCIH has even less of a reason to exist now than it ever did before, but it's not going away. As long as Dr. Briggs remains in charge, it is likely to continue in the mode that this draft strategic plan describes. I can live with that. Unfortunately, Dr. Briggs will not always be in charge; someday she will move on or retire. Her successor might not be as dedicated to trying to avoid wasting resources studying pure quackery as she has been. That's why the ideal solution would still be to defund and disband NCCIH. Until that happens, this strategic plan is probably about as good as NCCIH will get.
Meet the old plan. Same as the old plan. And comment. Your deadline is April 15.
Well, there were a few useful things there, as you noted. Hell, massage is useful in some applications, such as contractures or spasms.
Still, while I enjoy violations of the laws of physics as much as the next guy, I'll reserve that for watching drunks on holiday weekends defy the laws of momentum and gravity.
As in, try using woo to treat my nerve damage related pain, what I stick into that "practitioner" will most certainly not be an acupuncture needle. It'll either be a fist or a foot, ignoring the laws of physics by coexisting in time and space with an internal organ.
Oh, I neglected to mention, I'm also a chronic pain patient. I live on NSAIDs and the occasional analgesic, currently Tramadol (we rotate between Tramadol and codeine, at my suggestion, to avoid tolerance). Still, a bottle of 90 lasts me quite a while, as for me, PRN means just that, PRN pain.*
*Yes, I well understand the pain cycle, I've attended professional seminars in chronic pain management, surprising researchers by knowing their next step in research several times.
Those areas given low priority reek of protectionism, and by that I mean avoidance of studies on "natural" products sold in the marketplace and those commonly prescribed by naturopaths. Numerous products remain to be sufficiently examined in well controlled large-scale trials to determine efficacy and safety, and the dietary supplement industry knows it, even if the consumer does not.
It's disturbing that NCCIH is still focusing on improving symptom management, rather than zeroing in on The Root Cause Of Dis-ease, which as we know is a key strength of integrative/alternative medicine.
I'd say they are entirely correct to assign those three categories low-priority status. Without preliminary data showing that a proposed treatment might work, a sane IRB response to any proposed large-scale or "pragmatic" clinical trial should be along the lines of, "Hell, no!"
As for the other low-priority areas, yes, it's as if they don't want to know the answers: that acupuncture is basically a placebo treatment, or how you obtain genuine drugs from plant precursors.
Slightly O/T, but tangentially related:
If I recall, Sen. Harkin, the prime mover behind this monstrosity, was a big fan of bee sting therapy. This has suddenly become topical again since Gwynth Paltrow is recommending it. Ms. Paltrow is a talented actress and is considered by many to be very good-looking, but fortunately this has attracted a good amount of ridicule:
http://wonkette.com/600513/gwyneth-paltrow-want-to-put-bee-poison-on-he…
@palindrom
She (Paltrow, not the Senator) also wants you to steam your vagina and uterus - which of course is an "centuries-old Korean tradition".
https://drjengunter.wordpress.com/2015/01/27/gwyneth-paltrow-says-steam…
@ palindrom
Bee sting therapy?
Since the poor bee has to die to give you her* venom, that's not even a humane treatment.
If you have to get stung, I will also insist on this not being a topical treatment :-)
Trivia: it's true that bees do use their venom as a medical treatment. As part of their grooming, they occasionally lather themselves with a mix of saliva and venom.
Although in this case this is a topical treatment. Bees don't have a big brain, but they are not stupid enough to inject themselves with their venom.
* yes, her, not it. Honeybee workers/stingers are all females. The male bees are only good for one purpose**.
** if you really insist on a male bee to sting you, we are going into rule 34 territory.
Not that this topic has come up in my discussions with actual Koreans I know, and the only one who is close at hand is busy today (defending his thesis this afternoon)--but I'd guess that, like reiki, this "centuries-old tradition" dates back to the early 20th century AD, if not more recent. And to bring this back to topic, I suspect there isn't a whole lot of evidence for the efficacy of this treatment, which firmly places practical clinical trials in one of the low-priority areas Orac mentioned.
Amethyst @6 -- Well, parts of Gwynth are apparently held in high esteem.
Dunno if I spelled that right.
We'd better cut it out and get back on topic before our host gets mad at us.
If you want to understand the appeal of GOOP, it's instructive to survey its skincare section- especially the ingredients lists- and GP's fashion recommendations- especially Stella MacCartney.
The skincare is overwrought woo with a multitude of exotically named botanical substances- but with little focus on active ingredients- at exorbitant prices. The clothing is similarly insanely priced mediocrity by a celebrity ( of sorts).
Orac writes,
Meet the old plan. Same as the old plan. And comment
MJD says,
I did on the NCCIH site. Thank you.
While I do not consider myself to be especially cynical, I do understand that if one brays loudly enough about one's noble heart and one's great intentions then one can do what ever the f*ck one wants.
In harsh reality, objections to scurrilous practices can then be deflected as assaults on Motherhood and Apple Pie.
@Amethyst #6
Wife, raised in Seoul to a family that includes a prominent TCM "Doctor," is gaga for the woowoo but has never heard of this steaming the ladyparts business.
Now I fear that I have given her ideas.
As another chronic pain patient, this, and the new recommendations for pain management, makes me cringe. The American Psychological Association (hope I am remembering the organization correctly; by this time of night my eyes no liquidity never focus) said in their comments to the new initiatives that further research on what amounts to the placebo effects of complementary medicine need to be done so they can better be applied by psychological/psychiatric clinicians as a first line treatment for chronic pain.
Maybe I am cynical, but I feel insulted when professionals believe the best possible thing they can do for me is to pretend to treat me.
To those who are tempted to explain placebo effect to me, etc., please don't. My illness includes on-going, recurrint, visible tissue damage, which is one of the reasons I get frustrated that the documented pain from it is becoming a shrugged off, "Well, you'll have it for life, so just get used to it." In some studies, researchers have documented suicidal ideation in 25% of the patient population at any given time.
You'll hear no argument from me at all, Mrs Woo. I've had my fair share of suicidal ideation as well, with no significant clinical depression.
Some years ago, one of my Privates noticed me taking a codeine tablet and had the phenomenal lack of a survival instinct displayed by saying, "Pain builds character".
I kicked him in the shin - hard, then demanded that he stand still, as I wasn't done building his character.
He went to my superior, the First Sergeant and was laughed out of his office, he then complained to the Command Sergeant Major, who explained that I could have done far worse to him and a barked shin was getting off extremely lightly and by the way, I have some things you can take care of for me...
With that pain comes a spectacular case of bad attitude during a flare up.
..Strategic plan, objective, goals, whatever, it's all replete with weasel wording.
Makes you think that some of them in high places know exactly what they're about, but their salary depends on keeping up the facade.
"Hypocrisy is the tribute vice pays to virtue". Same applies with weasel words.
@ 15
What was the Private's name - Pyle? Because that seems to have been a very Full Metal Jacket-esque moment!
Probably some of your doctors fear, quite reasonably, that you would become addicted to your pain meds. It's a real issue, and a big part of why oxycontin is so hard to obtain in the US even with a prescription is the lengths people would go to to obtain it (including armed robbery) after becoming addicted to it. OTOH, there are ways to manage the pain. A good doctor in this situation will have you rotate among various analgesics, so that you aren't on a particular painkiller long enough to develop an addiction.
There are lots of people who repeat the old chestnut, "No pain, no gain." Most of them ignore the corollary: No brain, no pain. It sounds like this private was in this group. I hope for his sake that he acquired enough of a brain to learn his lesson, but that's far from assured.