
One of the most common tropes used by antivaxers is to attack herd immunity as not being real. Herd immunity, or as its sometimes called, community immunity, is a name for a phenomenon in which in a population with high levels of immunity to a disease members susceptible to the disease are protected. Basically, because the vast majority of members of the population are immune to a disease, that disease can't gain a foothold in the population and lead to an outbreak or an epidemic. Basically, transmission from person to person is interrupted because any susceptible person who becomes infected is surrounded almost completely by people who are immune. Thus, although individuals or small groups of individuals can become infected, in a population where a sufficient percentage of is immune the immune population serves as a "firebreak" on outbreaks, preventing them from spreading too far, protecting both those who are vaccinated and those who are not.
In this day and age, herd immunity is almost always achieved not through natural infection, but rather through vaccination. It's why public health officials emphasize high levels of vaccine uptake. How effective herd immunity is depends upon how infectious the agent being vaccinated against is, how effective the vaccine is, and what percentage of the population is protected by it. For instance, for a disease like measles, which is among the most contagious of vaccine-preventable diseases for which the vaccine is greater than 90% effective, the percentage of the population that needs to be vaccinated to achieve herd immunity typically from 90-95%.
So why would herd immunity be such a threat to antivaccine beliefs? The reason is simple. It's another major benefit of vaccines. More importantly, the existence of herd immunity undercuts another favorite antivaccine talking point, which is that, by choosing not to vaccinate their children, antivaxers are not endangering any one and that vaccinated children have nothing to fear from their unvaccinated children, because they are protected. Of course, obviously one problem with that argument is that many vaccines are not 100% effective, which is another reason why why herd immunity is so important.
Sadly, we see evidence of this effectiveness when vaccine coverage falls. Antivaxers will frequently point out that vaccine coverage in a state is at a very high level, and that's frequently true. However, it is pockets of low vaccine uptake, where vaccination rates fall below that needed for herd immunity in communities where antivaxers are concentrated. But what would happen if vaccine uptake declined nationwide? Well, a recently published study out of Stanford University asked that question. Basically, it was a study modeling what would happen under various scenarios if vaccine uptake. The reason is obvious:
The routine vaccination of children is declining in Texas and other areas of the United States where they allow for personal belief and other nonmedical exemptions to childhood vaccination requirements. In these areas, there is growing vaccine hesitancy—defined as a delay or refusal to accept vaccination based on personal beliefs despite availability— that could accelerate gaps in vaccine coverage across the United States. The determinants of the parental decisionmaking process on whether to vaccinate their child are complex and context specific, but are often influenced by misinformation, false claims regarding vaccine safety, and a low perceived risk of infectious diseases among other factors. While the sources driving vaccine hesitancy (eg, the “antivaxxer” movement, celebrity endorsement, and online content) have historically been outside of science and government, there have recently been calls for a special government commission on vaccine safety, despite overwhelming scientific consensus on the safety and effectiveness of vaccinations. If the panel were to draft policies that relax childhood vaccinations requirements, the already declining trends in vaccination coverage in US children may decline further. The aim of this study was to estimate the potential public health and economic consequences of declining childhood vaccination, a result of a growing vaccine hesitancy movement, using the case example of measles, mumps, and rubella (MMR) vaccination and measles virus.
I've written before about declining vaccination uptake in Texas. It goes counter to the inaccurate stereotype of antivaccine beliefs and vaccine hesitancy as being primarily the province of hippy-dippy, granola-crunching lefties in that antivaccine sentiment is driven by a potent mix of pseudoscience and far right libertarian anti-government regulation sentiment. Basically, antivaxers have figured out how to weaponize their views by coupling them to right wing rhetoric about "freedom." Not surprisingly, Dr. Peter Hotez, a pediatrician and public health researcher at Baylor and founding dean and chief of the Baylor College of Medicine National School of Tropical Medicine in the Department of pediatrics, is co-author on this study.
So what did the investigators do? Basically, they used publicly available data from the US Centers for Disease Control and Prevention to simulate county-level MMR vaccination coverage in children 2-11 years in the US. They applied a stochastic mathematical model, which was adapted to infectious disease transmission. Using the model, they estimated a distribution for outbreak size related to vaccine coverage. The predicted effects of declines in nonmedical exemptions were modeled and validated it against an independent data set from England and Wales.
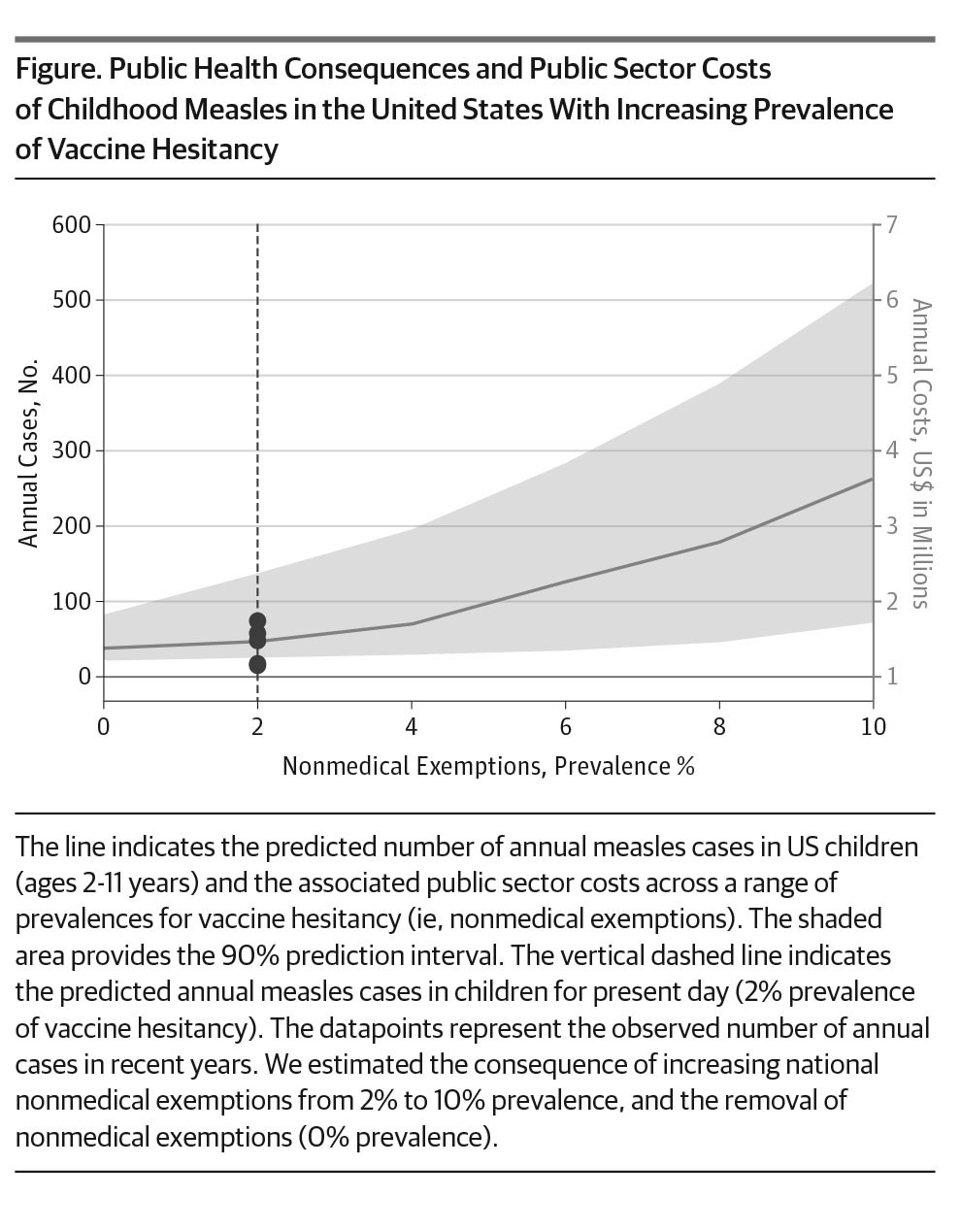
So what did the model show? Not unexpectedly, with increasing nonmedical exemptions comes increasing numbers of measles cases:
The authors also found:
We found that a 5% decline in MMR vaccine coverage in US children would result in a 3-fold increase innational measles cases in this age group, for a total of 150 cases and an additional $2.1 million in economic costs to the public sector (Figure).With declining vaccination coverage, the size of outbreaks increased. Increased MMR vaccine coverage in children, through elimination of children with nonmedical exemptions or other mechanisms, increased national MMR coverage to95%prevalence (state variation, 91%-98%).We predicted that this strategy would reduce annual cases of measles by 20% (from 48 to 38 cases) and was an effective strategy to mitigate annual measles cases and costs.
Basically, minor declines in MMR vaccine coverage (in this case, from 93% to 88%) can result in major increases in the number of measles cases. Indeed, the authors note that their model, if anything, probably underestimates how much the number of measles cases can increase if MMR vaccine uptake falls significantly:
This modeling analysis likely predicts a conservative estimate for a rise in measles cases associated with declining immunization status because of foundational model assumptions and since we limited our analysis to US children (age 2-11 years). The model is designed to simulate outbreaks in highly immunized population and nonendemic settings. However, large reductions in MMR vaccine coverage could allow for measles to become endemic again, which is not accounted for in this model, and would likely result in thousands of annual measles cases. Owing to constraints on data for immunization status in the adult population and social mixing structures, we limited our analysis to children ages 2-11 years who contribute approximately 30% of the annual measles cases. However, the number of cases of measles would be much larger when accounting for other age groups, such as infants, adolescents, and adults. This increased number would be, in part, driven by infants younger than 12 months who are not yet eligible to receive measles vaccines, as illustrated in the sensitivity analysis modeling an expanded age group (0-11 years). Finally, the upper limit of the prediction interval in the base case analysis demonstrated substantial nonlinearity, suggesting the possibility for large outbreaks due to random chance with small reductions in vaccine coverage.
This is an important point. As is the case now, even with high overall vaccine uptake over a wide geographic area (e.g., the state of California or Texas) there can exist pockets of low vaccine uptake where outbreaks can and do occur. It is not unreasonable to predict that if the overall vaccine uptake for the whole country declines from 93% to 88% there will either be more areas with vaccine uptake low enough to compromise herd immunity or that existing areas of low uptake will have lower uptake still, to the point where it's way below the level necessary for herd immunity. Then, of course, as the authors point out, the model doesn't even account for all the vulnerable children, such as those too young to be vaccinated, as was pointed out:
“Outbreaks happen in communities, so we need to zoom in further than just national or statewide statistics when it comes to vaccination rates,” said Maimuna Majumder, a researcher at the Massachusetts Institute of Technology in Cambridge who wasn’t involved in the study.
For example, one recent study in California found county-level measles vaccination rates as low as 70 percent even though the statewide average was 90 percent, Majumder said by email.
Whenever a study or public health official has expressed concern about low vaccine uptake in California, as in during the debate in 2015 over SB 277, the bill that passed into law and eliminated non-medical exemptions to school vaccine mandates in California, antivaxers have keyed in on that one statistic, that statewide vaccine uptake was high. While high average uptake is a good thing, if there are pockets where the uptake is well below herd immunity levels, outbreaks of vaccine-preventable disease become more likely. Fortunately, SB 277 appears to have been working well thus far. In just one year, there are fewer counties with exemption rates high enough to be concerning, and exemption rates overall have plummeted. No wonder antivaxers hate it.
Obviously, this is a modeling study, and a model is only as good as the assumptions used to construction and the data used to generate it. However, the results of this study are in line with what we already know. Decreasing vaccine uptake leads to more outbreaks of vaccine-preventable diseases, more cases, and more suffering among children. (Just look at the Somali immigrant community in Minnesota, where American antivaxers have convinced the Somali community that the MMR vaccine causes autism, resulting in a huge plunge in MMR uptake and the expected concomitant measles outbreak.) Antivaxers will try to deny that, but the evidence is overwhelming that vaccines work and that when antivaccine sentiments take hold children are endangered. If we're not careful, we could be sliding back towards a time when measles was endemic, as the UK did after Andrew Wakefield published (and publicized) fraudulent science that incorrectly concluded that vaccination with MMR was a risk factor for autism. The UK is only now recovering to the point that it was before Wakefield. If we're not careful, we'll be next.
It isn't rocket science - diseases just need access to hosts. Even a small drop can increase the "chinks in the armor" which allow diseases to be exposed to the vulnerable and enhance transmission.....
I saw a report on that same study on Ars Technica last night. I was wondering how long it would be before Orac blogged about it ;)
You listening, Jay? This is what your "alternate" vaccine schedule is risking. A three fold increase in measles cases with an approximate cost per case of $20,000 that could add millions in additional public health costs to Santa Monica (your taxes will have to go up to cover it).
And that's not even considering the human costs. Hmph.
Role of MMR II vaccine contamination with GAD65 containing chick embryo cell culture in the etiology of type 1 diabetes
http://www.bmj.com/content/358/bmj.j3429/rr
Q. Are transgender people a part of community immunity (a.k.a., herd immunity).
If the answer is YES, then transgender people should also be allowed to protect the herd through military service.
http://www.cnn.com/2017/07/26/politics/trump-military-transgender/index…
Hypocrisy destroys democracy.
The cost numbers also match other studies that looked at costs of outbreaks.
More evidence, if we needed any, that anti-vaccine activism costs us in suffering and costs.
I am skeptical Texas legislators would be affected enough by this, but who knows? The fact that Dr. Hotez is local might help.
Well, the Republican Party claims to be the party of fiscal responsibility.
Allowing the state to bear the burden of the paranoia of a few is not fiscally responsible. And I don't care what the libertarians say, this is not a personal liberty issue. No one has a right to infect other people.
Oh, Vinu. For a moment I was worried that the BMJ was posting nonsense. But then I checked and saw you were just hawking another of your silly "studies".
A friend suggested anti vaxers also anti Trump, possibly based on a legislature in Texas supporting anti vax. He and I both retired physicians have suggested it should be a legal requirement for parents to see that their kids are vaccinated.
Certainly should be anti Clinton which is purported to desire national Neal rules,but not a political,party item but a group who don't trust any medical science and are still seduced by Wakefield, Kennedy, and actors.
In history of U.S. Many splinter medical Groups and confidence men who follow the preacher and like to drink the Gatorade or cool aid..
Would that this discussion could,help those change belief.
@ Vinu (#3),
Thanks for sharing!
I've got absolutely no respectful insolence for your work, only curiosity and admiration.
Can someone please explain to me why, if this study is accurate, we don't have massive measles outbreaks amongst adults who long ago lost any immunity from their MMR vaccination? There are likely millions of adults in the US who are no longer immune to measles, not having had the MMR in well over 20 years, so you would think that for any small measles outbreak amongst kids, like the one in Disneyland, you'd also see many cases amongst adults over the age of 50 whose last MMR shot was likely over 30 years ago?
Wow, he has certainly taken the idea of self-reference to a whole new level....
@MB - because in most people, the MMR does confer lifelong immunity.
The fact that we don't have large outbreaks shows the efficacy of the MMR.
MJD, did you read the two comments on Vinu's "paper" that blows his I'll conceived "theories" out of the water and into the stratosphere? It might moderate your admiration.
Hint - if vaccines cause diabetes, why aren't we all diabetic? Another hint - anedoctal evidence. Yet another hint - no evidence that egg embryo cells contaminate vaccines. (Writing as one whose brekkies is two eggs on toast!)
Mr. Big @10: That's an excellent question!
The answer is that immune memory is not the same for all diseases. In general humans make very long lasting immunity to yellow fever, smallpox and measles. In general humans make crap, very short term immune memory to pertussis (whooping cough), both the disease and the vaccine. It's annoying.
The reason that the common "childhood" diseases were called that in the days before vaccines is that they were most often seen in children because if you got it as a child (and survived) you were very unlikely to get it as an adult.
That's how the idea of variolation came to be. Before any vaccines there was a process by which a person was deliberately exposed to a mild form of smallpox. They would get the disease, but generally a milder, more survivable form, and then would be protected against it in the future.
It doesn't work for everyone and every disease, but for the population at large, it does work. That's why we're here in the first place.
Thanks for asking!
Right now on Facebook a mom is debating me on the gardisil vaccine and is making crazy claims and getting likes for each crazy claim. I am so disappointed in humanity now. No facts, just emotional plea... then one mother said she only has one child (I only have one child) and will not take the risk... I remind her about Polio. The Disney debacle. She won't stop!!
My child is fully immunized. I recently had the shingles vaccine and while I had a reaction I would do it again! I was counting the days until insurance would pick it up. I have seen too many people suffer with Shingles. I may still get it, but I know it will be a whole lot easier having had the vaccine than not. I have no idea why these moms are so scared of vaccines. One mom claimed she had over twenty years in the pharmaceutical industry. I wanted to ask, in what position so badly but, I can't. My child is still connected to these weirdos.
Yeah, vinu what you've linked to is no kind of a research study, but a letter to the editor of the BMJ that you managed to get published on their website.
One of the comments on Research Gate to your "analysis" is too delicious not to share:
"I am not suggesting you need to run such experiments for a technical report, but I would seriously suggest that you take time to understand the biology of both vaccinations and type 1 diabetes."
Helen, it must be very demoralizing, but these people are doing bad research in the extreme wackadoodle corners of the internet. There are many articles (and comments) that demolish their concerns at Science Based Medicine and here. Recommend they look here. Then try to turn it off. But stand firm. Hang in there.
@ Panacea #2
Assuming we take Dr. Jay at his word, I doubt it's clear from the model what the risks would be if vaccination rates in X percentage of the population were only Y percentage, but only for children below the age at which Dr. Jay "advocates" for kids to get their shots – if the vax uptake was then appropriately high for kids age 3 and older...
We can't easily gauge the effect of pediatricians vaccinating on a delayed schedule as we can't just assume their patients would otherwise receive their shots on the recommended schedule. Parents with minor qualms about the MMR might vax on schedule if no doctor is available to recommend and provide the delayed service. However, parents with more qualms about the MMR might not vax at all unless some trusted physician avers "it's definitely safe if you wait a bit." If the later outnumber the former, the lax-vaxer pediatrician is actually aiding public health rather than harming it, at least in the short term. That might well be the case in localities prone to becoming anti-vax clusters.
For example, looking at the situation in the Twin Cities, I'd rather have Somali families immunizing their kids late than not at all. Since their freak-out is based on their unfamiliarity with ASD, and shock at having receiving several ASD diagnoses within their community, it would follow that this could be greatly relieved if the shots were delayed until after the age where ASD typically presents – hard to blame the vaccines then.
This does not mean that I'm willing to let Dr. Bob entirely off the hook for the Disneyland outbreak, or even give Dr. Jay a free pass unless/until he can verify that he doesn't enable non-vaxers and actually succeeds in getting otherwise reluctant parents to go along with immunizing on the delayed schedule. I'm just urging caution in judging any pediatrician who actually adheres to the practices Dr. Jay claims.( It seems pretty clear that Dr. Bob is an anti-vax enabler extraordinaire, handing out bogus medical exemptions and the like....)
MJD #9,
You are welcome.
Bovine serum albumin (BSA) contaminated vaccines and membranous nephropathy (MN):
In response to:
"Have you considered bovine serum albumin (BSA) contaminated vaccines as the source of both BSA and BSA antibodies in these patients?"
Dr. Du writes:
"That is a very interesting question I never thought about. Immunization of some types of mouse strains (e.g. BALB/c) with cBSA can induce MN-like kidney disease. ..."
https://www.researchgate.net/publication/51182667_Early-Childhood_Membr…
Dr. Pinheiro, an endocrinologist, commenting on my MMR/diabetes article:
"It´s very very interesting! The Increasing in type 1 diabetes in children last years must have an ambiental etiology and an etilogy could be antibodies against chicken GAD65 which cross-react with human GAD65."
https://www.researchgate.net/publication/317127703_Comparative_Pathogen…
I wonder if we are soon gonna see antivaxxers posting about the study, with this little excerpt interpreted as a call for a genocide of unvaxxed.
Helen, share where and we can come to back you up.
One other factor where waning immunity in adults would have a different effect on outbreaks to lack of immunity in children is the contact factor.
Most adults have less contact, and less intimate contact, with other people in their daily routine than do children. Children spread germs very effectively. Normal adults not so much, even less in asia where it is considered a good idea to wear a mask.
Good grief - will wonders never cease? MJD (#4) has said something with which I agree wholeheartedly.
*Goes for a lie down*
@Rebecca Fisher: yes, he said something admirable, then went back down his rabbit hole when he complimented Vinu.
@Vinu: Love the cherry picked comments. And the fact that you all go round and pat each others backs on all sorts of theories and don't so any real research.
@Craig, very true. There are certain circumstances that encourage the spread of disease. Day care, college dorms. Situations that aren't found in adults. There's a reason I refer to my young nieces and nephews as "The germ vectors."
Mr Big: Actually, a lot of adults over 50 had the measles virus, not the shot. There are ways to tell whether immunity has waned, and I think people who work in health care usually have blood drawn to check whether they're still immune. I'd suggest that should be expanded to adults who work in education and the military.
One of the major vectors of disease up until the '40s was the military, simply because that's what happens when you get a lot of people living together for long periods of time who have to share toilets, bunks,meals, do not get a lot of time for hygiene and are constantly under stress.
@PGP: I had the measles. I've had the MMR multiple times. I'm one of those lovely people who don't develop immunity to measles (fortunately, I did develop and maintain a rubella immunity from rubella - but I don't mind that it gets boosted with the MMR). Also didn't seroconvert with the Hep B series. My body is weird.
I get titers drawn and the new docs are always surprised...But - but- but - your medical records say you HAD the measles?? Yup. I depend on herd immunity. Thank you to everyone who seroconverts and protects me.
@PGP
Good point on testing education staff. The military probably not so much. New recruits get a shitload of vaccines which should cover any 'waners'.
MIDawn: Yes, I remember you mentioned that you have no immunity to measles. But most people do seroconvert. I recently had a blood test (I have anemia, and HIV screening is now mandatory, so I figured as long as I was there, might as well get tested for everything.) Next time I have a blood test, I might get my titers checked. Though my Mom and Dad both have measles immunity and I had all my shots.
But it can't hurt to double check, especially now that the Niblet is around.
Aside from the incoherent ("herd immunity") and off-topic parts, I take it.
On MJD (#4)
Actually, I don't understand what transgenders have to do with herd immunity. Being transgendered isn't contagious.
Perhaps it's my lack of unsterstanding of English, but the post doesn't make much sense at all.
@Renate, it's a reference to a news story that broke yesterday.
The Orange-haired, small handed pussy grabber has decreed that transgender individuals will no longer be allowed to serve in the U.S. military. This despite the fact that transgender people before undergoing transition, are disproportionately likely to enlist.
Re MJD's post -- leaving out the fact that it's another obvious hijack attempt on his part, I think we all agree with it.
Trust me, your command of English is better than MJD's.
Helen Hollis - hang in there and keep debating the anti-vax mommies. You may not change their minds, but your comments will be out there for others to read, and a few people who are wavering about the value of vaccination may well be convinced by your words.
As for the shingle vaccine, everyone should have it. My husband had shingle three months ago; he was very ill for a week and is still suffering with nerve pain and general weakness. So, in my experience, the vaccine is well worth it.here in the UK, it's only availble to those aged 70-80. I have some time to go before I'm eligible, but I'll be waiting at the surgery door the day after my 70th birthday!
Helen: let me add to Mrs. Grimbles encourgement. You won't change the minds of BSC people. But you may change the minds of people who haven't made them up yet. I have had people tell me they would have fallen for anti vax nonsense if I hadn't explained how the immune system works to them.
Vinu: that a couple of people might be thinking of a potential hypothesis based on a question you asked is not a ringing endorsement of your nonsense. Once these people sit down and read the literature, they're going to figure out its nonsense. Neither of those folks have any expertise in immunology.
PGP: nursing students have to show documentation of vaccination prior to starting nursing school. If you don't have your vaccination records, you can provide a titer as proof of immunity.
My mother lost my vaccination records at some point. Proof of immunity was not required when I first went to community college in 1983 because it was assumed if you graduated high school you were up to date. By the 90's, vaccine uptake had dropped due to the DTP scare, and outbreaks of vaccines preventable diseases had nursing programs a bit more cautious. When I went back for my RN in 1994, I was asked for records I no longer had, and got a titer which proved my immunity (I keep that lab record and have used it multiple times since as proof of immunity).
MI Dawn: I also have not sero converted to the Hep B series, which I've had twice. One employer wanted me to get it a third time, and I signed the waiver after that. I don't see the point of getting a vaccine I know won't take. If at some point an employer DEMANDS I get the series, I'll either have to get a letter from my doctor or do the series again . . . which of course will more likely than not fail again. But I'll do it to keep my job.
Honestly, I don't understand my co workers who wear a mask for six months out of the year rather than just getting the damn flu shot. So you might, I repeat might, get the icks for a couple of days. Still better than the mask.
Mrs. Gimble (# 37) writes,
I have some time to go before I’m eligible, but I’ll be waiting at the surgery door the day after my 70th birthday!
MJD says,
Hope your husband is fully recovered from the Shingles.
About getting the shot, tell them that you believe your "true" date of birth was at conception and maybe they'll give you the shot ~ 9 months earlier. :-)
Just trying to help!
Panacea--I got tired of wearing a mask so I get the flu shot. I also certainly have nasal carriage of many pediatric-office viruses which I bring into nurseries and NICUs in spite of that one rather ineffective but harmless flu vaccine. Therefore, when I do have a baby in the NICU, I will always defer to the neonatologists' daily exams and I avoid touching that baby myself. (All my other vaccines are, of course, up to date.)
Your post #38 is really filled with cognitive dissonance. There will soon be a third MMR recommended/required for those who don't convert after the first two. You should get that third Hep B series. I will waive the requirement for a smiley face icon here.
"In this day and age"--Orac . . . wow. I am in the midst of doing a completely hypothetical, retrospective and prospective study showing that a 5% decrease in studies like the one cited here will lead to nearly a 32% increase in fact-based decision making. I'm very disappointed to see you discussing this paper. Anyone who doesn't already believe that herd immunity is important is a clown and will not be influenced either by Hotez, et al or by you.
No cognitive dissonance here, Jay. In spite of my working in health care, I'm actually pretty low risk since I don't work directly in care delivery anymore. I don't start IVs much these days, I rarely give injections. I supervise my students doing those things. Once I become an FNP, I might be at a slightly higher risk, but still less than you'd think.
And regardless of my actual risk, if the medical literature were to suggest a third series would be advisable, I'd probably get it. But it doesn't show that, to my knowledge.
MMR on the other hand, is a disease with potentially deadly consequences. It's a vaccine everyone should get but there are still rare people like MI Dawn who will never sero convert. If there's evidence a third shot would reduce even those incredibly low numbers, and I didn't sero convert after two, then I'd go for the third without complaint. But if it still didn't work (and as MI Dawn points out, she HAD measles and still isn't immune) well, that's why herd immunity is so important.
I am allergic to tetanus. When I got a booster in 2003 after I got cut pulling an unresponsive patient out of a trashed motor vehicle, my entire left upper arm became very red and swollen, and the injection site blistered. In 2013, the local hospital required a pertussis booster for everyone who worked in the hospital, including nursing students and me, the instructor. We were in the midst of a local outbreak of pertussis, you see.
I couldn't find pertussis by itself. The pediatricians only had the DTaP. The health department didn't have it. My doctor wasn't sure he could get it, and he said it would be expensive and probably not covered by insurance even if he could get it.
He suggested putting me on a course of prednisone and Benadryl to protect against a possible allergic reaction from another TDaP, and I agreed. Because the plan made sense, and a booster was in my best interest anyway.
I could have gotten out of it btw. All I had to do was wave the ADA and demand reasonable accommodation. I didn't do clinic at the hospital in question, you see. I always did clinic at another hospital that wasn't asking for a TDaP booster. My manager wanted everyone to get it in case she needed me to go to that one hospital.
Nice try, Jay, but FAIL.
And while the flu vaccine could be better, I get it every year without fail . . . because the last two times I either didn't get it, or waited until too late, I got the full blown full flu: fever 103 F, aches, chills, the whole nine yards, and both times I got pneumonia and was sick for WEEKS.
Never. Again.
Recently on Barfblog.com there was a story concerning an anti-vaxxer group who lied to a school board about talking about organic fruits. Instead they showed an anti-vaccine video (article didn't say which one). The AVers are stooping pretty low to get out there message. It appears they maybe in trouble legally also.
Rich -
"The Courier Mail reports that the Miami State High School was deceived by the anti-vaccination activists, which is a common tactic:
ORGANISERS of an anti-vaccination documentary screening have allegedly tricked a Gold Coast state school into showing the film after telling officials they were running a seminar on organic vegetables.
The Gold Coast Bulletin also reports the deception by the AVN and Vaxxed:
ANTI-vaxxers ‘tricked’ a Gold Coast school principal in order to spread their inaccurate documentary, says a fuming Premier Annastacia Palaszczuk.
Premier Palaszckuk today slammed the lobbyists for misrepresenting the true reason for the meeting.
“My initial advice is that there has been misrepresentation from that organisation to the school in question, where they conveyed to the principal that it was to be conveying information about organic produce.
The ABC has also reported the deceit:
A Gold Coast principal was hoodwinked into hiring out his school hall for a screening of a controversial anti-vaccination documentary, Queensland Premier Annastacia Palaszczuk says.
“My preliminary advice is that there has been some misrepresentation to the school in question,” Ms Palaszczuk said.
“They conveyed to the principal that it was to be conveying information about organic produce.”
https://reasonablehank.com/2017/07/26/queensland-public-high-school-hir…
Mikema: New recruits get a shitload of vaccines which should cover any ‘waners’.
My bad. Other people have mentioned that, but I forgot it. Although I suspect I nailed the reason for the 'shitload' of vaccines.
Panacea: Yup. My mom's a nurse, and works with high-risk patients, so she had to do both.
Jay Gordon: All my other vaccines are, of course, up to date.
Sure they are, Mr. I-don't-give-the-MMR.
@ Renate
MJD isn't saying transgenders in general have anything to do with herd immunity. His analogy is between military service and herd immunity. Within herd immunity, we count on everyone to protect the community as a whole. We don't harm the community by excluding people we just don't like from participating in this protection. In his analogy, MJD is framing military service as also a form of community protection. Thus, excluding willing individuals from service because they're transgendered is as counter-productive as it would be to prevent guardians from getting their kids vaccinated because they happen to be transgender.
So i wouldn't say the post doesn't make sense, but that the sense it makes is rather outre, or stretched, or idiosyncratic. It seems to involve a very uncritical view of the U.S. military, but that's par for the course in discussing any social policy within the military, and within those brackets I wouldn't say MJD is totally wrong in the comparison...
At one of the hospitals where I'm on staff (and where health care workers are required to get flu shots to protect patients), one of the lab employees used to wear a mask all through flu season rather than get the flu shot. I can't imagine how people can stand doing that all day long out of fear or as a protest mechanism (there are of course exemptions for those with valid medical reasons).
Jay Gordon: "Panacea–I got tired of wearing a mask so I get the flu shot."
Good for you. Our recalcitrant lab employee finally got fed up too and decided it was better to get the shot.
"Jay Gordon: All my other vaccines are, of course, up to date.
Sure they are, Mr. I-don’t-give-the-MMR."
PoliticalPig--I give the MMR. My vaccines are up to date.
And, don't call me a liar or I'll call you a
@JustaTech
I don't think the current measles vaccine gives lifelong immunity. The CDC requires two MMR shots, so that would mean one shot does not lead to lifelong immunity. The CDC is silent in regards to the length of immunity after the second shot as far as I can tell.
As well, there are many adults who got the measles vaccine in the mid 60s, which didn't work, but didn't get natural measles either. Therefore they should not have any immunity to measles unless they've been vaccinated twice since with MMR which is unlikely. In Canada, the two doses of MMR wasn't implemented until 1996, so anyone vaccinated prior to that in Canada is likely no longer immunized. You'd think we'd see many adults that received the ineffective measles vaccine, or were vaccinated in Canada prior to 1995 catching measles from measles outbreaks, yet we don't, at least not like you would think given how contagious it is. Puzzling.
Panacea—My comments were unnecessarily snarky. If you work with needles, even occasional IVs and injections, Hep B is an important vaccine. I consider it more important than the MMR but that’s open to debate.
Decades ago, there was a single pertussis vaccine (whole cell) and the demand was very small so manufacture stopped. We need it back again because, like you, some people develop adverse reactions to tetanus vaccination.
I need to change my "name" to "Totally Traumatized"! Went to corner store for ice cream and there was a SUV with a big decal on the rear window "The biggest lie in history is that vaccines are safe and effective."
I'm poleaxed! Never saw that before.
PGP #28
Back in the Good Old Days of the Spanish War and the AEF, people loved to talk about the hardiness of the good old frontier boys and their superior marksmanship - having grown up on shooting down bears and coyotes and Indians - but the Army quickly learned to quarantine such regiments in barracks until anyone who was going to die from one or another common ailment died and stopped being a burden to the organization.
#48 Mr. Big:
CDC supplied info on measles vaccine:
https://www.cdc.gov/vaccines/pubs/pinkbook/meas.html#vaccines
"Duration of Immunity
lifelong
...
vaccine-induced immunity appears to be long-term and probably lifelong in most persons. "
.
.
Note it was only the 1963 killed vaccine that was ineffective and there has been live attenuated vaccine produced since 1963 (Edmonston B) followed by the live further attenuated Schwarz strain in 1965, finally settling on the live more attenuated (Moraten) Edmonston-Enders strain in 1968.
https://explorevaccines.wordpress.com/2011/04/03/name-that-strain/
and:
https://www.cdc.gov/measles/about/history.html
.
There aren't a lot of folks wandering around who haven't been infected with wild measles or haven't received at least 1 dose of a live attenuated vaccine.
Robert I Bell: Back in the Good Old Days of the Spanish War and the AEF, people loved to talk about the hardiness of the good old frontier boys and their superior marksmanship – having grown up on shooting down bears and coyotes and Indians – but the Army quickly learned to quarantine such regiments in barracks until anyone who was going to die from one or another common ailment died and stopped being a burden to the organization.
One of the more interesting features of the Spanish Flu was the more robust your immune system was, the more likely you were to die. As far as the 'robustness' of the fighters of the Spanish War go, no one ever remembers that Theodore Roosevelt was actually fairly sickly for most of his early life.
Jay Gordon: Oh, stop it. You were a lying misogynist snake a few years back and you're still a lying misogynist snake. You think a few glib quips will make people forget your history. Doesn't work on me, jerk. I still remember the time you went after Lilady, and the internet never forgets.
Maybe you give the MMR now, probably not.But you only give it because you were pressured to, not because you made the decision on your own. And even now, you're still willing to risk your patient's lives by waiting three years. I don't even know why you became a doctor. Helping people is the last thing on your mind. You should have been a mercenary.
Therefore, when I do have a baby in the NICU, I will always defer to the neonatologists’ daily exams and I avoid touching that baby myself. (All my other vaccines are, of course, up to date.)
1. ...and the neonatologist somehow has magically different nasal carriage than you? C'mon...lame excuse. If you want to examine a baby then (a) don't be actively sick, (b) don't pick your nose, and (c) wash your damn hands well before doing your exam.. You do understand germ theory, don't you?
2. Defers to neonatologist's exam because: (a) won't get paid by insurance anyhow for doing his own exam in NICU, and (b) probably won't get paid by family for cash-pay billing for NICU exam, and, (c) NICU infants are almost always never old enough to examine for the purpose of telling parents they don't have to vaccinate based on his own personal experience which trumps all science.
@Mr Big #48:
FTFY. And it doesn't matter what you think (or more correctly, want to believe). What matters is what the evidence says. And given that adults vaccinated as children don't get measles, it works.
There is a difference between less effective and completely ineffective. That early measles vaccines were less effective than later ones doesn't mean they were ineffective.
See comments above about less effective vs ineffective. In addition, community immunity is very good at preventing measles from jumping to immunologically naive patients.
TL:DR You are just another antivaxxer downplaying the effectiveness of vaccination as a tool to stop disease and using tactics and tropes we've seen and refuted literally dozens of times before.
@Rich & @shay,
Just for clarity, the 'tricked high school' was in Australia (not Florida) and they (of course) showed Vaxxed.
The Vaxxed morons seem to be having difficulty booking venues. (Yeah!) In some cases ticket holders don't know the venue until 2 hours before the showing to reduce protests.
I love how anti-vaxers try to claim that the MMR isn't effective by waving their hands & making all sorts of assumptions - yet Rubella, for instance, has been eliminated from the Western Hemisphere, and a country like Mexico has as close to ZERO measles cases as you can get (and the US, despite a population of more than 300 Million people, has no endemic transmission of measles either).
So, what's their explanation for this? Well, to them, it couldn't possibly be that we have a highly effective vaccine & still an extremely high rate of vaccination as well......as opposed to say, Europe, where, in some countries, vaccination can be spotty - resulting in epidemics of tens of thousands of cases.
Jay Gordon: "Decades ago, there was a single pertussis vaccine (whole cell) and the demand was very small so manufacture stopped."
How many decades ago are we talking about? The DTP vaccine was licensed for use in 1949.
I doubt vaccination safety will be enhanced by employing a whole-cell pertussis vaccine which kids would presumably receive on a separate visit to the pediatrician ($$ from the additional office visit might look attractive to certain peds, and could be sold as lowering the Vaccine Toxin burden as compared to the combined vaccine).
@Mr Big: In case you missed it *I had the measles*. The holistic, honest-to-goodness "you'll get lifetime immunity if you get this" measles as a child. I also got (because my grandfather was a GP and strongly believed in vaccines) every form of vaccine that came down the pike (recommended for regular patients, not things like yellow fever) while he was in practice. (He SAW all the horrible things that can happen to kids/families with VPDs so he was strongly pro-vaccine. We also had autism in our family BEFORE vaccines expanded beyond smallpox).
I don't seroconvert. My MD thinks I *may* be OK if measles breaks out here even without a MMR, but I'd much rather not take that risk at my age. And, like Mrs Grimble, I'm counting the years till I can get the shingles vaccine, which is 60 years old here in the US
@Lawrence: and, of course, neither the US nor Mexico have areas where there are lots of poor people living in slums with lousy diets, bad water, poor food and shelter like those *OTHER* countries that have horrible measles outbreaks with deaths....oh wait....
(/sarcasm, just in case it's missed)
#55 Julian Frost said, "There is a difference between less effective and completely ineffective. That early measles vaccines were less effective than later ones doesn’t mean they were ineffective."
Yep... and the live attenuated vaccines weren't even less effective. In fact the 1st one was more effective but caused more unwanted side effects (fever, rash) than the later versions... kinda' like the whole cell pertussis vaccine vs. the acellular pertussis vaccine.
.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1227617/pdf/amjphnation000…
EDMONSTON B AND A FURTHER ATTENUATED MEASLES VACCINE-A PLACEBO CONTROLLED DOUBLE BLIND COMPARISON
George Miller, M.D.; et al.
Aug. 1967
Note seroconversion rates of the various vaccines - Table 5, page 1337:
"Edmonston B - 97.6% seroconversion
Further attenuated (Schwarz) - 95.8% seroconversion"
.
No surprizes. The less attenuated Ed. B invoked a stronger immune response than did the further attenuated (further weakened) Schwarz strain - see Fig 2.
Both provided very good seroconversion rates and titers so anyone vaccinated with them that did seroconvert is probably immune for life.
.
So much for the anti-vax trope that there are huge quantities of older and elderly who are not immune to measles because of the 'poor performance' of the 1960s vaccines.
My sister doesn't seroconvert for chicken pox, and three people in my immediate family have had shingles (my dad, and my maternal grandparents). Fortunately, I'm adopted, so probably not susceptible to that myself, but I really wish I could get the shingles vaccine early anyway. My sister has had chicken pox twice and has been vaccinated three times, no results.
I also know someone who is naturally immune to smallpox. She also lived through the 1950 influenza epidemic that killed two of her brothers within three weeks of each other. (She was also the only surviving child of a set of triplets, so she is an only child who should have been one of five.) And she was born during WWII in southwestern Ontario, Canada, so we're not talking about the 19th C. here, or someone who lived in a developing country or something.
I was in the cohort that got a possibly-defective measles vaccine here in Canada, so a couple years ago I got revaccinated. I came down with bronchitis a few days later, but I don't think it was related, although I wondered at the time.
Since children have started getting immunised routinely for HiB, I no longer get horrible sinus infections that go from nothing to catastrophic in a matter of hours and spread like wildfire to my ears, throat, and chest. That used to be an at least semi-annual thing for me, and nearly killed me when I was in graduate school in 1999, since it turned into pneumonia along with the sinus, ear, and throat infection. I can't prove those two things are related, but I feel they are. Theoretically, HiB is supposed to be one of those things you only get once, but...
Re: "neither the US nor Mexico have areas where there are lots of poor people living in slums ". From what I read, Mexico has 97% vaccination rate for measles and similar rate for other diseases. They keep track of every child, and if a child is late, then the nurse visits the home and vaccinates the kid right there. If parents are at work, the nurse does it anyway then leaves paperwork with a babysitter. Nurses visit slums as well.
@kitty: that was my point. Mexico (and the US) have some horrible social problems in some areas. But with high levels of vaccinations, those children aren't dying of measles like we see in other countries.
@Julian Frost
"FTFY. And it doesn’t matter what you think (or more correctly, want to believe). What matters is what the evidence says. And given that adults vaccinated as children don’t get measles, it works."
Whoa, a little pedantic aren't we? Lol...Sorry if I said "I think" instead of "the evidence presented by CDC vaccine researchers...blah, blah, blah". What are you, a first year med student or something? Lighten up there pal.
"There is a difference between less effective and completely ineffective. That early measles vaccines were less effective than later ones doesn’t mean they were ineffective."
Sorry, but I was quoting directly from the CDC page which states that the measles vaccine from that era "was not effective", so you are, in a word, wrong.
"This recommendation is intended to protect those who may have received killed measles vaccine, which was available in 1963-1967 and [b]was not effective[/b]."
If you are going to play Mr Pedantic, perhaps you should check your own facts before making a fool of yourself. Or not.
"TL:DR You are just another antivaxxer downplaying the effectiveness of vaccination as a tool to stop disease and using tactics and tropes we’ve seen and refuted literally dozens of times before."
Off your paranoid delusional meds again?
Oh, G-d, not Philip Hills.
@Mr Big #65, whom I suspect is Travis:
I notice that you didn't link to this CDC Page in any of your comments. Link, please.
This, Travis, is why you keep getting caught out.
O RLY? You mean this? Let's review your comment, shall we?
Where is this "quoting directly" part? This?
"If you received a measles vaccine in the 1960s, you may not need to be revaccinated. People who have documentation of receiving LIVE measles vaccine in the 1960s do not need to be revaccinated. People who were vaccinated prior to 1968 with either inactivated (killed) measles vaccine or measles vaccine of unknown type should be revaccinated with at least one dose of live attenuated measles vaccine. This recommendation is intended to protect those who may have received killed measles vaccine, which was available in 1963-1967 and was not effective."
How many, Chuckles? Would a picture help?
One blessing of multiple chronic health issues: my PCP uses the ones he can to let me get shots early. Trying to remember if I was able to get the shingles vax yet. I know I did all the pneumococcal ones.
Oh, I doubt that.
Here we go:
@Julian Frost
Sorry, here you go.
http://bfy.tw/D6mv
Didn't realize you were so inept at this interwebz stuff. I should have known based on your mostly fact-free posts. My bad.
^^ Risky click of the day, Mr Big. Why the link shortener??? Without letting the site run scripts (Noscript is your friend, people), it looks like dodgy garbage.... It is *imgtfy.com* and it looks like a site to show people how to 'Google' like your five years old.
Mr Big, #72: Julian asked for a link to the source you used, which you claim to be CDC. You responded with a LMGTFY link for a sentence entirely different from the one you had uttered and attributed to CDC.
Are you too inept at this interwebz stuff to give a link to your source, or are you expecting Julian search through all the CDC pages to try to divine the one you used? I understand it's easier for you that way, since when Julian finds your quote to have an entirely different meaning when placed in context, you can reply that it's the wrong guess on his part.
That's why citations are required when claims are made.
Thank you Tim and Se Habla Espol.
@Mr Big #72, when I asked for a Link, I meant a link to the actual Page on the CDC Website you claimed you were quoting from. Posting a link to LMGTFY is not proof.
Ahem.
@MI Down - sorry, I missed it. You are absolutely right.
On generic vaccination topic. I am in my late 50s, yet somehow managed to miss getting chicken pox as a child. For some reason, "childhood diseases" passed me by. Other kids in school got them. Got it at the age of 32 instead, it was no fun, and it's possible - though, obviously, not definite - that my POF was somehow related given that symptoms started shortly after. Of course, correlation isn't causation and all.... But still, with the vaccine had been licensed just a few years earlier. The kid I got it from was current on all vaccines, but this one wasn't yet in use.
Having just gotten through early Lyme - still finishing up antibiotics, was lucky enough to get the typical rash. made me read up again on the vaccine. I could vaccinate my cats for it if they had been going out, but not myself. Big thanks to anti vaxxers and lawyers.
Just to butt in about Hep B vaccine courses:
Jay Gordon to Panacea:
Jay, Panacea has had 2 full courses of Hep B vaccine and not responded serologically. That's 6 injections, FYI. The MMR primary course is 2 shots, and if someone sometime determines that it should be 3 shots (who has said this?) then that has no relevance to the situation with Hep B or Panacea's situation.
Panacea should not just get another standard Hep B vax series as you suggest. After 2 failed attempts, this would not work. He probably need not worry if he gets exposed - he may be protected anyway via anamnestic immunity.
If he really needs to gain documented confirmed seroconversion for work purposes, the options are for him to get a high dose (40mg/ml) series IM, and if that fails, to get a course of high dose (40mg) vaccine via 5 intradermal shots 2 weeks apart.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4621464/
Dingo: She ;) I'm a girl.
Thanks for linking to the article. I was not aware a high dose Hep B vaccine was available. I always decline the series since my second set did not sero convert me, but I've lost the documentation of the 2nd series (a job I had 17 years ago, so Employee Health likely doesn't have it either). So if I do get an employer who just insists, this gives me an option that at least has a chance of working instead of wasting time and money on a series that won't.
Looks like "Mr. Big" has learned the lesson that APV learned a few years back (http://scienceblogs.com/insolence/2014/12/05/no-the-cdc-did-not-just-ap…) - if you provide a link, people will notice if you lie about what the link says, so you're better off just lying, and refusing to provide a link.
Wow, didn't realize that commenters here can't even follow a link or do a web search. If I provide a link, will I also have to describe where on the page the text is located? Should I include a short tutorial on how Internet Explorer works, what a hyperlink is and what a mouse is? I know the page was the first result from a Google search using the quote, but I guess even that was too taxing.
https://www.cdc.gov/vaccines/vpd/mmr/public/index.html
@kitty
A Lyme vaccine can't work. You can catch Lyme disease every summer your entire life, never acquiring immunity from it. If you want to dose yourself with Osp A and try and do the community a favor by disinfecting your local ticks using your own blood, have at it. Let us know how you get on.
Should I include a short tutorial on how Internet Explorer works, what a hyperlink is and what a mouse is?
Yes please, could you please come here to help me figure out how to install Internet Explorer please?
I have a hard time making it run on my system.
Alain
Alain: Why would you want to run explorer on your system?
Way to miss the point. Anyone can make a claim and then say "search for yourself" when challenged to provide proof. You did not (at first) post a link to the CDC page when asked for evidence. Around here, if you make a claim, it is your responsibility to provide supporting evidence.
It wouldn't help. I'm using Chrome.
As for your link, if you had been reading the comments carefully, you would have realised that Narad in #68 posted the exact same link and pointed out that you misquoted what it said. It's the word "here" that's coloured blue.
@PGP #83: I think we need to have a "Sarcasm" sign a la The Big Bang Theory for you. Alain was being sarcastic. I have worked out from some of his other comments that he uses Linux. Internet Explorer (and its follow up Edge) doesn't run on Linux.
A Lyme vaccine can’t work.
Evidently Big Vet hasn't received the message.
JF: Computer illiteracy strikes again.
That's OK. Nobody really gets Explorer to run well on their system anyway.
They don't even make it for the Mac anymore (thank god).
An op-ed commentary on the Stanford study appears in today's Wall St. Journal.
Generally a good piece, with one groaner - parents who refuse vaccination for their children on various grounds are referred to as "conscientious objectors" in the war against infectious disease.
In reality, these parents (and especially the hardcore antivaxers and antivax physicians who urge them on) are a fifth column working to bring vaccine-preventable diseases back into prominence.
PGP,
Julian is right, we need a sarcasm tag; a very subtle one.
Alain
"As for your link, if you had been reading the comments carefully, you would have realised that Narad in #68 posted the exact same link and pointed out that you misquoted what it said. It’s the word “here” that’s coloured blue.'
Yup. Narad seemed clueful enough to easily find it, why couldn't you? I quoted directly from the CDC web page. That's why "was not effective" is in quotes, see? Couldn't be simpler.
I can only guess that commenters here are so rabidly obsessed with vaccine promotion, that even when the CDC itself says one isn't effective, extreme cognitive dissonance sets in, and you become unable to even do a simple search to confirm. Sad. Science requires no sacred cows. Vaccines, at least on this supposed "scienceblog" clearly are one, to the point where even when the CDC admits a vaccine didn't work, y'all argue otherwise. Kind of pathetic, really. Keep your confirmation biases at the door.
Apologies accepted.
Why would anyone apologize?
You said "many" people vaccinated in the 1960's were vaccinated with an ineffective vaccine. You also said the MMR doesn't confer lifelong immunity.
Narad showed you how that statement is wrong. The ineffective vaccine was used in a four year time frame. Note that ineffective doesn't mean NEVER effective. So the CDC recommended a booster with the newer MMR.
The statistics show a dramatic drop in the number of measles cases starting in 1964 (when the ineffective MMR was being given). That drop flattened out near zero with a couple of minor bumps. After the 2nd dose was recommended it went to ZERO and native measles was deemed eradicated (meaning the only measles in this country comes in from somewhere else).
The system worked exactly as it should. Continuous monitoring of vaccines identified a vaccine that wasn't living up to expectations (not dangerous, just not working well), replaced it and recommended a booster for those who got it.
NO WHERE in there is any evidence the CDC thinks the MMR does not confer life long immunity. If it didn't, measles would be endemic in ADULTS as the immunity wore off. We'd have seen a big spike in adult measles cases in the 80's and 90's among the VACCINATED population.
We didn't see that. We have every reason to believe the MMR confers life long immunity.
I got my MMR in that time frame, btw. I am immune to measles.
!
!!
Only after the fact, which is to say, your buffoonish intellectual dishonesty is in front of limelights that you turned on all by yourself.
@Mr Big #91:
Quoted directly? As Narad showed in #68, you took what was written there out of context and then "added" to it. You took the fact that there was a killed vaccine that the CDC found was ineffective and said that people vaccinated against Measles in the 1960s were no longer immune. But you omitted that there were attenuated Measles vaccines available contemporaneously with the killed vaccine, and that these were over 95% effective.
You lied by omission and you were busted.
"This recommendation is intended to protect those who may have received killed measles vaccine, which was available in 1963-1967 and was not effective."
Not really sure how you can somehow read that this quote from the CDC and think it means something other than what it says. The 1963-1967 measles vaccine was "not effective". Not partially effective, not mostly effective, not even somewhat effective. It was "not effective". IE: did not protect the recipient from the measles.
Clearly the vaccine indoctrination by commenters here is so strong, that even when a manufacturer admits that a vaccine is "not effective" the confirmation bias kicks in and commenters try and ridiculously make claims as to what "not effective" really means. What's next? What the meaning of "is" is?
They shouldn't call this site scienceblogs, since it appears that bloggers/commenters here have little understanding of what science really is.
*sigh* In the 1960's two main vaccines became generally available in the US and UK for the first time. One was a live vaccine. It worked really well, but it had side effects. The other was the inactivated vaccine you refer to.
There were reports of a measles like illness, especially when someone got the live vaccine after the inactivated one. There were varying reports on how long immunity lasted.
The problem really wasn't that the inactivated vaccine wasn't effective. It's that it wasn't as effective as the live vaccine because no one was really sure how long the immunity would last. The process worked the way it was supposed to and that vaccine was abandoned in favor of one that had side effects but was more reliable. The number of measles cases dropped like a stone, and later MMR vaccines finished the job. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4007870/
What you've tried to claim is that MODERN vaccines don't confer life long immunity based on this one inactivated vaccine and that's simply not true.
Despite one of the first two vaccines being ineffective or at best only moderately effective and soon dropped, the other was very effective and was replaced by another effective vaccine in 1965.
Measles incidence dropped considerably in the next few years and then went to almost zero when a second dose was added.
If the vaccine weren't effective or immunity waned, we would see periodic like we do with pertussis and mumps.
@Mr Big #97:
Once again, you lie by omission. As has been pointed out several times already, there were several vaccines in use in that time period. One (a killed vaccine) was not effective but the others had seroconversion rates of over 95%. To repeat Reality's comment #61:
I think its clear that you don't understand what a "lie by omission" is. The attenuated measles vaccine that was sold in the mid 1960s didn't work, was not effective, however you want to put it. Everybody knows this, so you can quit arguing a simple, well-known, well-documented fact. Immunity didn't last more than a few months, leaving the person with no immunity. If you got that vaccine, and didn't get the measles, then you are likely walking around today with no immunity.
I apologize if somehow that intrudes on whatever magical fantasy you've built up in your head about vaccines, but here in the real world where science lives, we don't cheerlead, we look at evidence. If a vaccine or medicine doesn't work, we don't paper over it and continue cheerleading like you do, we do something about it.
Mr Big @101: Why do you assume that the people who got the killed measles vaccine never got any other measles vaccine?
That specific one didn't work and was removed from the market. Why do you think that the people who had gotten it never got another measles shot that does work? That doesn't make any sense at all.
Also, how many people are we talking about anyway? A thousand? Ten thousand? Fifty?
There's a lot of relevant data missing and you've made some unsupported assumptions.
Ahem....
Measles epidemiology and vaccine use in Los Angeles County, 1963 and 1966
Mass measles immunization in Los Angeles County
And then about ten years later:
The Benefits From 10 Years of Measles Immunization in the United States
So in other words, what Chris is saying is measles immunization worked even back then. Which is what I said.
And we did do something about it. We fixed it. That's why we got to ZERO native cases of measles around the turn of the century. The measles cases we have currently came here from other countries.
The surprising find in the Los Angeles county study (one study, two papers), was that there was a definite shift in epidemic trends, even though the vaccine coverage was limited.
Community immunity was in play, which is part of why the effect of a not very effective vaccine was muted. Though some suffered years later, like Dr. Snyder:
https://sciencebasedmedicine.org/measles-gets-a-helping-hand/
By the way, those who are old enough to the get not so great vaccine are well over fifty years old. I don't hear much about a measles epidemic among baby boomers.
Mr Big you seem to be making a mountain out of a mole hill. The slice of the US population that may have been affected by the less effective vaccine would be in their early fifties at this time (I had measles prior to the vaccine). Most the affected population either had the measles at some point in time or had the more effective vaccine later. Also, even though I had the measles when I was young, 30 some years ago while coaching a 3/4th grade basketball team I contracted the measles again. The only affect from the second case I got the measles rash (spots) but otherwise was fine.
If you so worried about measles vaccines, look at many parts of the world where measles are either endemic or pandemic. Maybe you should help do something about that.
@Mr Big #101:
Did you not read Reality's comment #61? Here is the relevant part of it.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1227617/pdf/amjphnation000…
EDMONSTON B AND A FURTHER ATTENUATED MEASLES VACCINE-A PLACEBO CONTROLLED DOUBLE BLIND COMPARISON
George Miller, M.D.; et al.
Aug. 1967
Note seroconversion rates of the various vaccines – Table 5, page 1337:
“Edmonston B – 97.6% seroconversion
Further attenuated (Schwarz) – 95.8% seroconversion”
I've bolded the key part. The (attenuated) Edmonston B vaccine had a seroconversion rate of 97.6% while the Schwarz vaccine, which was further attenuated, had a seroconversion rate of 95.8%.
So in "the mid 1960's", there were two attenuated measles vaccines being used, and each had a seroconversion rate of over 95%. Cut it how you like, that IS effective.
Mr Big #101:
You have been informed the vaccines were over 95% effective, so what is left is the 5% of individuals who received these vaccines in the mid 1960s and who did not develop protective immunity.
They would comprise what percentage of the adult population today... less than 0.1% maybe?
@Panacea #41 --
I'm several days late, but please accept this standing ovation for a wonderful response to Mr. Cognitive Dissonance. : - )
#109:
Now I understand what you mean by "lie by omission". I guess you accused me of that so quickly because it is obviously your strategy of choice. You posted remarks about 2 measles vaccines, but [b]omitted[/b] the killed, ineffective measles vaccine, which like I stated above was "not effective".
That's pretty much the definition of a "lie by omission". Nice try, but you ain't foolin' anyone. Not sure why you would even lie about such a thing. Are you employed by the vaccine industry? I really can't think of any other reason why you would try and lie about something that is easily found on the CDC website, as well as many other health websites, pubmed, etc. Why attempt a cover up of a well known fact that happened 40 years ago? Bizarre.
Mr Big @112: I'm confused. What is your point again?
A vaccine was made. It was found to not be as effective as desired. It was removed from the market 60 years ago.
And?
Like, those are the facts, no one is arguing about that.
So what is your point?
"So what is your point?"
My point, clearly elucidated above, is that there are likely to be adults walking around without immunity to measles, since they got an ineffective vaccine during a period of low measles outbreaks. Ineffective measles vaccine + no measles = no measles immunity.
What is your point? Do you have one beyond defending the vaccine industry at all costs no matter how many lies of omission it takes? It doesn't seem so. I'll have to find other websites to get truthful vaccine information, since this website seems to play fast and free with the truth.
Mr Big why don't you worry about the children that have idiot anti-vaxxer parents that will not get them vaccinated. The total of at risk children for measles is far greater than the small population of fifty year olds that have some risk of contracting measles. It appears your moniker doesn't apply to you thinking ability.
Mr Big: "My point, clearly elucidated above, is that there are likely to be adults walking around without immunity to measles..."
Which is why that anytime there is a measles outbreak it is suggested that those born in 1957 and later check their vaccine status. Since I was in the era of that dodgy vaccine and there was no one around to tell if I had had measles, I got an MMR a couple of years ago.
So, seriously, you don't have much a point to those who can actually figure out simple algebra.
Moreover, the "clearly elucidated" "point," as it were – wholly lacking in quantification as it is – wholly ignores the basics of SEIR models.
What I keep wondering about is this:
" In Canada, the two doses of MMR wasn’t implemented until 1996, so anyone vaccinated prior to that in Canada is likely no longer immunized.[*] You’d think we’d see many adults that received the ineffective measles vaccine, or were vaccinated in Canada prior to 1995 catching measles from measles outbreaks, yet we don’t, at least not like you would think given how contagious it is. Puzzling."
Well, what's so puzzling? That one's premises may be a crock of sh*t? Was this supposed to introduce some sort of gushing evolutionary river of sh*t? It seems to have gone nowhere.
[*] "Vaccination is not immunization" trope duly noted.
"Like, those are the facts, no one is arguing about that."
If that's true, why are all these commenters arguing?
Because, "Mr Big", you brought up the irrelevant issue, and kept harping on it.
Get over it.
Because you keep making the same wrong point over and over, Mr. Big.
Chris, you probably didn't need a booster. An MMR titer would have told you if you had immunity or not. That's what I got when Mom lost my vaccination records.
@Mr Big #112:
>blockquote>You posted remarks about 2 measles vaccines, but [b]omitted[/b] the killed, ineffective measles vaccine, which like I stated above was “not effective”.The reasons I didn't bring it up is because
a) it was already acknowledged;
b) it was not germane to the point I was making.
In #10, you asked:
Lawrence and JustaTech pointed out that (in general) the Measles vaccine or Measles component of the MMR Vaccine conferred lifelong immunity and PGP mentioned that most over 50's got Measles and were thus immune.
In your comment #48 you argued that the second shot proved that the first shot on its own was not enough, and then you wrote:
Begging for the ability to edit or preview my comments.
@Mr Big #112:
The reasons I didn’t bring it up is because
a) it was already acknowledged;
b) it was not germane to the point I was making.
In #10, you asked:
Lawrence and JustaTech pointed out that (in general) the Measles vaccine or Measles component of the MMR Vaccine conferred lifelong immunity and PGP mentioned that most over 50’s got Measles and were thus immune.
In your comment #48 you argued that the second shot proved that the first shot on its own was not enough, and then you wrote:
Reality responded at #52:
In #61, Reality gave the effectiveness of the Edmonston and Schwarz vaccines:
“Edmonston B – 97.6% seroconversion
Further attenuated (Schwarz) – 95.8% seroconversion”.
You then proceeded to misrepresent what the CDC said, among other things.
As for your question to me “Are you employed by the vaccine industry?”, no. I work for an IT development firm.
In #114, you finally laid out your argument.
The bottom line is this:
1) In 1963, two vaccines against Measles were introduced. An ineffective killed one and the highly effective Edmonston B attenuated vaccine. In 1965, the attenuated and also highly effective Schwarz attenuated vaccine became available.
2) Not everyone vaccinated from 1963-1967 was vaccinated with the ineffective killed vaccine. Many were vaccinated with either Edmonston B or Schwarz.
3) After the ineffectiveness of the killed vaccine was discovered, it was withdrawn (in 1967) and most (if not all) of the people who had received it were revaccinated with one of the more effective attenuated vaccines.
Your initial argument was and is wrong.
Panacea: "An MMR titer would have told you if you had immunity or not."
Hmmm, the choice to walk down to the local pharmacy and pay $50 for a shot from a teeny tiny needle. Or make an appointment with my doctor, get a blood draw and pay for lab tests that would not be covered by insurance... more than $100.
Plus the fact that I got mumps for a second time, and it is popping up again.
How do I choose?
"That’s what I got when Mom lost my vaccination records."
My mother died when I was eleven years old, and my dad is clueless.
"get a blood draw"
From a much bigger needle. Also, last blood draw causes a bruise that lasted more than a week.
The irony, it burns. Let's review the actual comment by "Mr Big" that engendered Julian's purported "lie by omission":
Whoops, "Mr Big," dismayingly, seems not to know the difference between "attenuated" and "killed" [sic], or if he does, chose to double down with tedious bluster over his own error.
The original link was broken by the mystery SB prefixing. The paper is here.
Aaargh. Thanks.
And I had checked it in another window. I try to do this before posting a link, because some have retreated behind a paywall or were moved elsewhere.
One of my favorite studies comparing pertussis outbreaks versus vaccine policy has been moved multiple times. The last one is to the site of one of the authors:
https://www.researchgate.net/profile/Robert_Chen7/publication/13631420_…
What I like about that is it has a nice clear account of why this claim (which I saw posted yesterday elsewhere) is an idiotic lie: "What about SIDS. Japan has almost no incidents of SIDS / the lowest rates in the world. They delay vaccinations until 24 months!"
(my luck, even without extra html, that link will be borked)
I got hit by this SB weirdness not too long ago, as well. It seems to have been fixed.
^ Just to explain in more detail, this is how the original link came through:
h[]tp://scienceblogs.com/insolence/2017/07/26/surprise-relatively-small-decreases-in-vaccine-uptake-can-lead-to-big-increases-in-vaccine-preventable-disease/comment-page-1/www.ncbi.nlm.nih.gov/pmc/articles/PMC1435674/pdf/pubhealthrep00160-0015…
The real link was there, but SB prepended itself.
^^ And, in fact, that "http://" was added auto-craptacularly when I tried to paste the original. I, for one, prefer my comments to be delivered as entered.
Narad, the rules of HTML and HTTP differentiate between local links and global links. A link that starts out with a
//, possibly preceded byhttps:(or another protocol specifier) is global; otherwise, it's local. Local links don't work very well world-wide, so many blogging engines convert them to global ones. The result that WP gave was the global version of the local link you gave it.That is just too much weirdness, and annoyances. I muck them up enough all by myself!
"and most (if not all) of the people who had received it were revaccinated with one of the more effective attenuated vaccines."
Citation? That sounds like wishful thinking. My guess is that they didn't. Things were different back then, we didn't have internet, etc, so most people likely had no idea the vaccine was not effective and pulled. The other two vaccines you mentioned were also pulled off the market, which commenters omitted to mention for some reason.
It's not wishful thinking. It's what happened. We know this because measles rates dropped so precipitously. If these folks hadn't been revaccinated, we'd know from infection rates.
The other two vaccines were pulled off the market because they were replaced with a better vaccine. That happens; we get a perfectly good vaccine, but maybe it has side effects. We develop a newer one that produces the same or similar immunity, but has fewer side effects. So we switch.
Vaccines undergo constant review and revision.
Heck, even Andrew Wakefield was developing a new MMR vaccine.
Please just don't do the grandmother, eggs, suck, how to, thing, really. It can autolink if it wants to (and in the past, I've had to poke it with a stick to see when it would), but it's never OK to add characters to a comment.
That would be "the internet" that still documents that your previous tantrum amounted to pouring a bucket of shіt over your head in public, right?
@Se Habla Espol: I'm also not finding an RFC with this global/local rule that you mentioned.
Narad, what I called 'global' is referred to in the specs as 'absolute'; what I called 'local' is 'relative'. Try rfc 1808, "Relative Uniform Resource Locators". There may be a more recent rfc on the subject, as usual.
Some people swear by them, others swear at them. WordPress seems to be in the latter category.
@Mr Big #133:
Internet no, but we did have etc. When inoculations were given, the lot number and type were recorded against the recipient. Although harder than today, it would not be impossible to find out who was vaccinated with the killed vaccine and get them revaccinated when they came for a doctor's visit. All the Health Department would need to do is send out letters to every doctor's office and clinic.
As I mentioned above, letters from the Health Department to every clinic and doctor's office, and that would be handled.
Not mentioned? Reality @ #52.
So it was mentioned. And the Moraten strain is still exceptionally effective.
Looks like RFC 3986. Thanks, but note that I haven't read it yet.
"Hmmm, the choice to walk down to the local pharmacy and pay $50 for a shot from a teeny tiny needle. Or make an appointment with my doctor, get a blood draw and pay for lab tests that would not be covered by insurance… more than $100."
Yes. Also consider time it requires to get the test results including the appointment to get tested which may be important if you are traveling e.g. to Europe now or there are cases locally.
I am in my late 50s, and until very recently I'd been 100% sure I was vaccinated against measles as I was vaccinated against everything required as a kid. But after reading on this blog about measles in Europe- I am traveling there in a couple of weeks, I suddenly started to wonder. After some reading, it turned out in the country I grew up in, the measles vaccine was only introduced in 1968. While they consider people my age probably immune because of that, I wasn't really sure as I knew I hadn't had measles. Somehow childhood diseases - other than rubella - passed me by, I even only got Chicken Pox at 32 (not fun).
The doctor suggested a titer test first - this was a couple of weeks ago. I actually was thinking of just getting the shot, but figured it'll be just a few days and I was curious especially as a friend in the same position tested positive for antibodies. Also, in my state pharmacists aren't allowed to give MMR. Well - it took several days to get an appointment - as the doctors were booked and nurse practitioner out on vacation - to send me for titer test, and the clinic requires an appointment before it. Then, apparently, there were a few days to get the results. It turned out, no, I am not immune. Interestingly, I was immune to other diseases. Rubella was no surprise just shows the diagnosis at the time was correct, but I was sure I hadn't had, yet I got a pretty high antibody count - in the hundreds. Probably had a very mild case - I remember other kids in my school class getting it, I just didn't get sick enough to notice.
At any rate, I did get my MMR shot today, now hope, I have enough time to get immunity, but CDC tells two weeks, so it's OK. Hopefully, I'll not get high fever or anything just in time to board the plane. BTW - I credit this blog with telling me about measles in Europe.
@Mr Big "A Lyme vaccine can’t work. ..." It works for dogs. No, I am not planning asking my vet for it... there is a company now working on the version for humans. Also, the first Lyme vaccine produced in 1994 reduced new infections by 80%. Sure it wasn't perfect, but it was working, and yes, I know that antibodies don't provide immunity, but the way the particular vaccine worked was effective.
@Panace
"It’s not wishful thinking. It’s what happened. We know this because measles rates dropped so precipitously. If these folks hadn’t been revaccinated, we’d know from infection rates."
With no citations, that's exactly what it is: wishful thinking. I guess you commenters only demand evidence when it suits your confirmation bias? Otherwise, anecdotes like this one are just fine? You are mistaking correlation with causation. Just because measles infections went down, you can't claim it was just automatically because of the vaccine. That's marketing, not skepticism and certainly not science. Measles cases also went down prior to the release of the vaccine. Are you going to give MMR credit for that as well?
@kitty
"It works for dogs."
Great. I am not a dog.
"No, I am not planning asking my vet for it… there is a company now working on the version for humans. Also, the first Lyme vaccine produced in 1994 reduced new infections by 80%. Sure it wasn’t perfect, but it was working, and yes, I know that antibodies don’t provide immunity, but the way the particular vaccine worked was effective."
The current vaccine being worked on is similar to LYMErix, namely dosing you with Osp A to hopefully disinfect the ticks that attach to you. Unfortunately, the actual effectiveness of LYMErix is unknown, because the Lyme disease test was changed when it was released to ignore the proteins the vaccines were created from. That's one of those tricks where you can make a vaccine look like it works by changing the testing for the disease. That's just dishonest imho.
But here's a question for you. Why bother dosing patients with Osp A to hopefully disinfect attached ticks when you can just make a typical vaccine that creates antibodies to the germ itself, like MMR, and many others?
Yawn. Before the 1960s just about every child had measles by at fifteen:
The Clinical Significance of Measles: A Review
Then something happened, and it pretty much disappeared in the USA (except for imported case):
From http://www.census.gov/prod/99pubs/99statab/sec31.pdf
Year.... Rate per 100000 of measles
1912 . . . 310.0
1920 . . . 480.5
1925 . . . 194.3
1930 . . . 340.8
1935 . . . 584.6
1940 . . . 220.7
1945 . . . 110.2
1950 . . . 210.1
1955 . . . 337.9
1960 . . . 245.4
1965 . . . 135.1
1970 . . . . 23.2
1975 . . . . 11.3
1980 . . . . . 5.9
1985 . . . . . 1.2
1990 . . . . .11.2
1991 . . . . . .3.8
1992 . . . . . .0.9
1993 . . . . . .0.1
1994 . . . . . .0.4
1995 . . . . . .0.1
1996 . . . . . .0.2
1997 . . . . . . 0.1
" because measles infections went down, you can’t claim it was just automatically because of the vaccine."
If the 90% drop in measles between 1960 and 1970 in the USA was not from vaccines, please enlighten us with an alternative reason. Provide citations.
"If the 90% drop in measles between 1960 and 1970 in the USA was not from vaccines, please enlighten us with an alternative reason. Provide citations."
Sorry, that's not the way science works. You can't make claims, then ask others to disprove them. That would be like me saying that measles cases went down because of better hygiene. You disagree? Then prove it wasn't better hygiene, with citations.
You've made the classic mistake of assuming a correlation is causation.
"Then prove it wasn’t better hygiene, with citations."
We cannot prove a negative. But I can ask you what fantastic hygiene change occurred in that decade to cause an airborne disease plummet. Explain exactly how measles plummeted. I already gave you in comment 103 what happened in Los Angeles county with the measles vaccine.
We really want you to tell us the alternative reason. Come on! Entertain us!
Do not mention deaths. Do mention any other decade, unless it was at least a 90% drop. Do not mention any other disease. Do no mention any other country. In short: don't change the subject.
Oh, and about that "hygiene" hypothesis (otherwise known as a really wild guess), I shall present this evidence: Measles vaccine coverage and factors related to uncompleted vaccination among 18-month-old and 36-month-old children in Kyoto, Japan
It says:
So what hygiene crisis happened in Japan in 2000 to cause measles to become common, and deadly? Provide citations.
@146
So you can't prove a negative (which actually isn't true, you can) but you expect me to? That's not the way science is done. You can't just assume a vaccine works, you need actual data, not just a correlation. Again, you are mistaking correlation for causation.
I figured at a site called scienceblogs, folks would know how basic science is done. You can't even assume having antibodies means you have immunity these days, as sometimes that isn't the case, and people get the disease even though they have antibodies. Science is tricky.
Come on! Answer the questions!
Why did the incidence of measles in the USA plummet 90% between 1960 and 1970?
And what "hygiene" crisis in 2000 caused measles to rise and kill so much in Japan?
Sorry Chris, that's not science. You have it backwards. You have to use data to prove something is true, not just assume it is because something seemingly correlated occurred. My uncle had a heart attack while eating a cucumber sandwich. So I guess cucumber sandwiches cause heart attacks right?
The way you seem to think it works is that you make a claim, and if no one else can refute it, then it must be true. I guess God must exist, because you've claimed he does, and I can't prove he doesn't. Lol...I wish it worked that way but in the real world it doesn't.
I gave you data. At least four different PubMed indexed papers. I can't help it if you don't understand it.
Here is some more:
Impact of Vaccines Universally Recommended for Children—United States, 1900-1998
Evolution of Measles Elimination Strategies in the United States
Now what data do you have that hygiene caused measles to plummet in the USA between 1960 and 1970?
And what hygiene crisis happened in Japan to increase measles incidence so much in 2000?
"I guess God must exist, because you’ve claimed he does,..."
Oh, you are a special kind of idiot. Did you just get fired from Google recently?
@150
Hmmm...it appears you're simply indulging in ad hominem. Typically, that's the last bastion of a person with no argument, which appears to be the case here, since you have no data supporting the claim that those that got the ineffective measles vaccine in the sixties were revaccinated at some point later. Its also clear you can't tell the difference between correlation and causation so there is little point in further discussion about how science works. I suggest enrolling in a science class to see what its all about.
The pro-vaccine argument runs something like this.
The scientists who developed measles vaccines in the 60's predicted those vaccines would be effective in reducing incidence of measles based on similar efforts against smallpox, diphtheria and polio.
Despite the ineffectiveness of one of the vaccines, that prediction proved true as shown by the numbers Chris cited. The effectiveness was further increased by adding a second dose of the measles vaccine, which reduced incidence to near zero and eliminated endemic transmission of measles in the western hemisphere.
The effectiveness continues to be shown by recent outbreaks like the Disneyland case and the Minnesota Somali community outbreak which were started by nonvaccinated individuals traveling abroad. In both cases people who were not vaccinated were much more likely to get the disease than others who were vaccinated.
Your original argument was that one of the original vaccines was ineffective and you were very worried about these vulnerable individuals contributing to an outbreak. Based on 50 years of experience shown in Chris's data, that hasn't been a problem.
We might share your concern if you could cite an outbreak where vaccinated individuals were equally likely to get the disease as non-vaccinated. Or show a recent case (last 10 years) where even one of the people getting the disease had only received the 1963 ineffective killed vaccine.
Mr Big @147 You said you can prove a negative.
Please do.
While you are at it, please definitively prove that none of the people who received the ineffective measles vaccine ever got any other effective measles vaccine for the rest of their lives.
"Based on 50 years of experience shown in Chris’s data, that hasn’t been a problem."
Again, correlation does not imply causation. Don't take my word for it, look up the terms correlation and causation and see what you find.
I"ll start you off:
https://en.wikipedia.org/wiki/Correlation_does_not_imply_causation
I'll give you a concrete example. My senile grandmother was having a mouse problem in her house. So she decided to put out a bunch of mouse traps, but forgot to put bait in them, so of course they didn't catch anything. My not senile grandfather, meanwhile, had an exterminator over to clear up the problem. However, since my grandmother hasn't seen a mouse since she put out the unbaited traps, she claims that the mice saw the traps and all decided to leave the house lest they get trapped. I don't have the heart to tell her the traps had no effect on the mice. So even though the mice all disappeared soon after she put out the traps, correlation doesn't imply causation. Does that help?
Mr. Big: "Hmmm…it appears you’re simply indulging in ad hominem."
No. It was an insult. I did not dismiss your comment for what you are, but what you said. Which was pretty nonsensical. Especially your total dismissal of the given data. Plus your little story about mice and your grandmother is entertaining because it shows you do not have a clue.
So exactly why did measles incidence plummet 90% between 1960 and 1970 in the USA?
And what "hygiene crisis" in 2000 caused measles to return to Japan and kill at least 88 kids?
Don't knock yourself out with all that hand waving.
@153
You dIdn't take university maths I assume. Proving a negative can be easily done using a proof by contradiction among many other methods. For centuries it was thought possible to square a circle. However, it has been proven impossible. In other words a proof was created that proves a negative, that squaring the circle cannot be done.
As to your other claim that all recipients of the failed measles vaccine were subsequently vaccinated with a successful vaccine, so therefore have lifelong immunity, all I would need to do is find a counterexample: IE: One person who received the failed measles vaccine that didn't get any further measles vaccinations and also didn't get measles. Not hard to do at all with the right resources.
Regardless, science requires proof of something (or not something). You can't just say because my uncle had a heart attack while eating a cucumber sandwich, that cucumber sandwiches cause heart attacks. Even if you knew 1,000,000 people who had heart attacks while eating cucumber sandwiches, that's still not proof that cucumber sandwiches cause heart attacks, just like saying measles cases went down after a measles vaccine was introduced doesn't prove that the measles vaccine was the cause of fewer measles cases. Science doesn't work that way. If we banned cucumber sandwiches, and the rate of heart attacks also happened to go down, would you then also then claim that's proof that cucumber sandwiches cause heart attacks?
It's always fun to watch people like Mr Big step into an argument. He's apparently developed a series of routines which allow him to sidestep questions. We've already seen the 'ad hominem' routine, the 'correlation does not equal causation' routine and the 'you don't know science' routine. (There may be more, but I'm not in a manure-shoveling mood.) The common factor that all of his little intellectual autoeroticism routines seem to share is that Step #1 is to reject the data.
Indeed. Now all that's left is to see if Mr. Big is really Travis. We'll know soon enough, I'm sure.
"Proving a negative can be easily done using a proof by contradiction among many other methods."
Ha, ha, ha, ha, ha! That is hilarious. This is not about the four color map problem. This is pure statistics. You don't have a clue. But your little stories are hilarious.
I take it that "Mr Big" has elected to skip copping to his disastrous "lying by omission" self-soiling.
Ah yes, more ad hominem. The last bastion of those who have no argument. I guess it can be frustrating to try and argue when you don't have the science education to back it up, but you should try and refrain from it as it tends to have a boomerang effect, no matter how many of you pile on.
You're greatly overestimating Travis J. Schwochert's creativity, IMNSHO.
This:
https://i2.wp.com/freethoughtblogs.com/pharyngula/files/2017/08/science…
Where would that be?
It is hilarious in that this guy does not understand words he attempts to use. I don't see an ad hominem. Nor do I see any actual math from him. I am laughing at him.
The overarching issue is that he's dishonest. If you're going to accuse someone of lying when your own words plainly demonstrate that it is in fact you who was in the wrong and then compound the problem by (1) trying to ignore its being pointed out and (2) bitching stupidly when item 1 is pointed out, you're not worth the time of day.
But his little stories were just so darn cute!
I am sorry, between this thread the one at Pharyngula about the idiot that got fired from Google, I can't stop laughing.
Sorry, but pathetic attempts at cyber bullying don't disprove science, no matter how much of it there is. You can all pile on with more ad hominem, or whatever immature games you care to play, but it doesn't change the facts.
I'm saddened that most commenters here have nothing better to do than troll other commenters with ad hominem. Me, I'm headed back to the lab to do some work after a much deserved break. I'll have to go elsewhere for an answer to my question regarding cucumber sandwiches it seems, since no commenters here seem to understand basic logic or science.
"I’m headed back to the lab to do some work"
After the lab test be sure to do a cat scan.
I take it that the "boomerang effect" will be kicking in promptly once "the lab" of "Mr Big" catches wind of the intellectual degeneracy of the RIgulars.
So laughing at Mr. Big's lying and that he still does not know what "ad hominem" means is now cyber bullying. It was certainly a good thing I was not drinking anything. Snort!
Mr. "Big": I had already given you a citation on measles rates, if you'd bothered to read it. Post #98: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4007870/
Chris also gave you multiple citations on this. Really, dude. Learn to read.
And now we see that there is a loop counter somewhere amongst all the other sub-routines: "If loop count = n, then initiate flounce routine."
Oh dear. Science doesn't work what way? I take it your "lab" has nothing to do with epidemiology, biomedical nor statistics.
Panacea: " Really, dude. Learn to read"
Then Mr. Big whines "But that is too hard!"
Science Mom: "I take it your “lab” has nothing to do with epidemiology, biomedical nor statistics."
That is my bet also.
@Mr Big:
Sure you are. And I'm flying my private jet back to O. R. Tambo International Airport having watched yesterday's eclipse.
I guess I'm in the minority, but I think Mr Big does have a lab.
.
Based on his screen name and his comments here, my supposition is that it consists of a basement bedroom, an inflatable sex doll, a copy of Vaxxed and a penis enlarger.
I would wonder whether Mr Big's lab has had its rabies vaccination.
If Mr Big is worried about cyber bullying, perhaps he should close his Sarahah account. I just read it's used for that a lot.
On a more serious note, we could have looked at things that increased in the 60's like watching color tv or reading Spiderman and the Hulk and looked to see if there was a correlation. But instead, we in effect did real science. We made a prediction that a mass vaccination against measles would reduce the incidence of measles and then tested it by actually doing it. And guess what? It worked!
We've unfortunately also done the reverse test in several places with bad consequences.
If Mr Big thinks vaccines are the mousetrap factor (obvious but wrong), he should at least propose a plausible candidate for the hidden exterminator factor.
And if he really thinks vaccines had nothing to do with it, why all the hoo-rah about one ineffective vaccine 50 years ago?
It reminds me of people who keep talking about a paradigm shift which will magically change reality into the way they think it is despite the data.
Real paradigm shifts don't change the data. They just change the way we understand and explain them.
And whether it was vaccines or some hidden factor, what we did in the US in the 60's obviously worked.
#168 where he says our comments "don't disprove science" is especially funny because he never cites any science we have failed to disprove.
Sorry, Mr Big, but science shows that the measles vaccine is very effective and very safe.
And we ignore that at our peril.
Opus@177,
With handcuff and rope?
Alain
Alain,
Handcuffs and ropes are generally used with real people. Um, or so a friend tells me.
Of course, there's an xkcd for that.
I was going to just make the obligatory David Carradine/Eli Wallach Circle of Iron reference here, but then W—dia told me this:
Mr Big @ 156:
Hahahaha! I am genuinely wiping away tears I'm laughing so hard. Oh my goodness.
Yes, I have taken university math. I've studied math that would make you stomach churn and your eyes cross. I've taken classes that involved the phrase "Start by visualizing a point on a 5-dimensional hypercube".
And that's just the math I've done. The math I've seen? It would make Lovecraft weep in fear.
So don't tell me about math. I bet you're one of those people who thought Fermat's last theorem was trivial.
But all of that is beside the point. Proofs in math are totally disparate from proof in science.
Hypercubes are more than what I have ever done. Though I have done some topology (heat transfer, which I hate). I also read math books for fun, including Simon Singh's one about Fermat's last theorem.
Yes, Mr. Big's comment was totally hilarious.