
The news is bleak. I don't have a lot of confidence in the reported numbers. At one time it was said that on a nice Saturday in the summer, four out of five cars driving around in downtown Boston were looking for a parking place. This is somewhat like the situation in Liberia and possibly other affected areas. There may be as many Ebola victims driving around in taxis looking for a clinic as there are in clinics. Or maybe a fewer. Or, maybe more. Maybe a lot more.
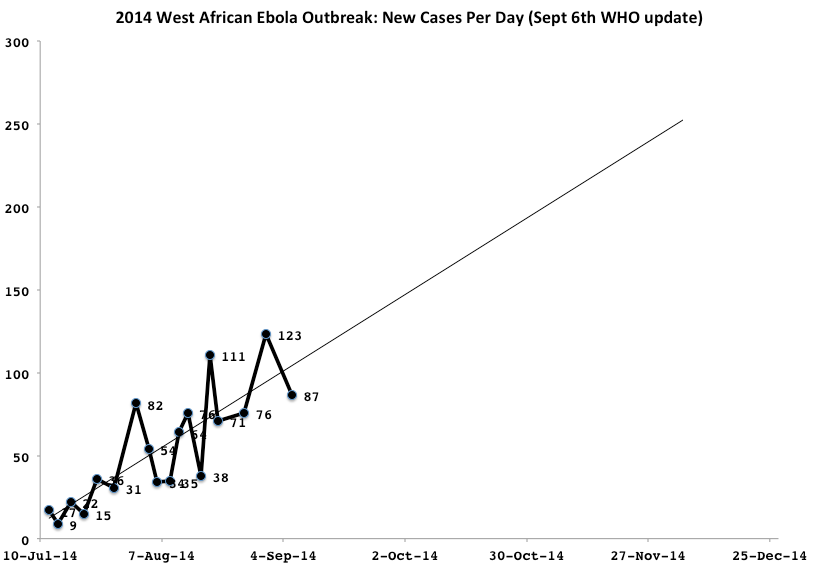
But, we have to work with the data we have. There are two charts based on the information provided by WHO for up through September 6th. I've projected each data set out 90 days. Since there is no abatement in frequency of new cases, and in fact the number continues to increase on average, and since WHO is claiming that the situation in the worst hit areas is pretty much out of control, a 90 day projection seems reasonable. In other words, there is no reason to think that the relative rate of new infections is going to change because of any outside intervention or internal change in the situation.
The first chart shows the number of new cases. This varies a great deal from report to report. Some of that variation over time is probably real, reflecting the internal complexities of disease spread. But I suspect it is mostly administrative. If a bunch of cases don't get into one report, the get into the next report. This explains a nearly perfect alternation between increase and decrease between successive reports.
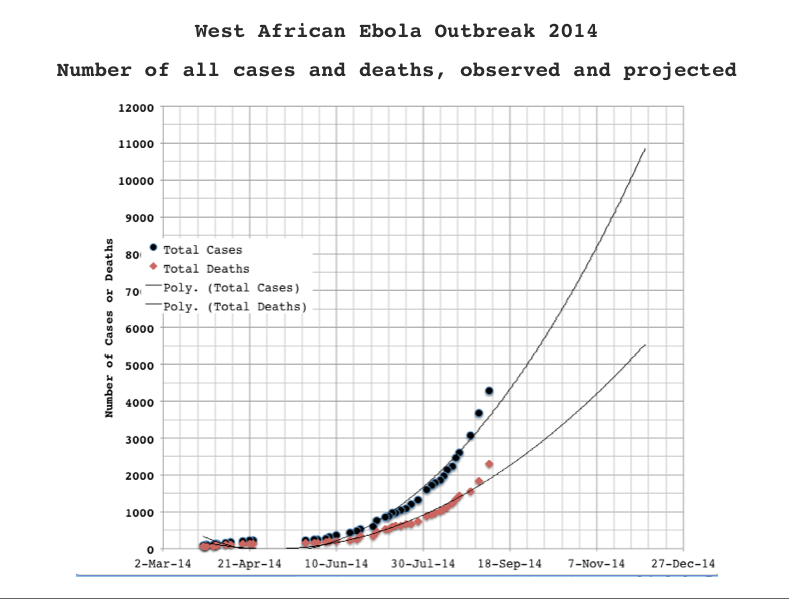
The second chart shows the number of cases over time, accumulated. This Projected outwards, we can guess that by around the beginning of 2015, there will have been over 10,000 people who have been infected by Ebola in West Africa (including Nigeria and Senegal as well as the main area of the outbreak), and over 5,000 deaths. Since I know you are curious, if this is projected out over a year or so, the number of infected people goes to between 60,000 and 70,000. I have no idea if this is realistic.
The situation is bad and getting worse.
Perhaps I've missed it - our semester has started, bringing with it all the usual foul-ups - is there any explanation for why this outbreak has gotten out of hand, grown so quickly, spread so far so fast? Did it begin in a more populated region, or has the amount of travel between these regions grown greatly since the last outbreak?
Both. Mainly, though, it is the size and density of the population.
I listened to a discussion on NPR last night (possibly the night before) with someone from WHO, someone from doctors without borders, and a few others. I was driving home from school and caught only the final 30 minutes of it but: none of the people in the discussion had anything optimistic to say about the chance of getting a handle in it in any reasonable amount of time. It was more than a little depressing.
It was some time ago that this outbreak began to look unique in terms of the length of time and the generations of inter-human transmission with no reduction in contagiousness. Ebola infects so many cell types within the human body that its evolution usually isn't focused on transmission between hosts, but rather transmission between cells within a single host. This is the same reason that HIV doesn't learn new tricks, even though it rapidly mutates. Now we're seeing this Ebola have some kind of genetic plan for getting to the next host. It's evolving instead of just mutating.
I don't think so. For one thing, mutating is evolving. Also, it can not have a plan.
Dean: That's my impression as well. Whatever Liberian health system may have existed was wiped out during the civil war, and the maximum response WHO could launch was anemic.
It turns out that there really is no plan if there is an outbreak. Ebola, of all the known scary diseases that actually happen is in some ways the easiest to contain.
How worried should we be that it will mutate as it spreads? That is, it can mutate--but what conditions would make that more probable? Is just the spread of the virus making that more likely?
sounds like Andromeda strain and for sure the more people get infected the more the virus has the opportuinity to become more virulent
I don't think of Ebola as a mutate-and-change type of virus. It does evolve as any other virus does but underlying genetic variation does not equal surface changes in functionality. There is a real threat of an airborne version arising because we know this is functionally possible.
We hear a lot about rapid evolution of viruses and big changes that make them very deadly all of the sudden. But that actually hardly ever happens, and when it does, it happens more often in different kinds of viruses other than Ebola.
Having said that I think we have a different problem. The CDC and the WHO, which are the organizations that are supposed to swoop in and stop outbreaks, have demonstrated that this isn't really a thing. They just can't do that when conditions are bad. And conditions are usually bad, frankly, around the world. So that whole thing where the guys in space suits show up and fix everything? Fiction.
ebola is made of RNA strands RNA is known 2 undergo rapid genetic changes. Nucleotide substitution resulting from high error rates in process of RNA synthesis.
These projections look ok at a rough approximation.
The linear regression of new infections that you draw gives a linear equation. ( y = A.x )
Therefore the volume of total infected by your method by integration assumes a 2nd order polynomial ( y = B.x^2 )
However you have to consider that the rate of infection is a direct relationship to the population size - this makes it an *exponential* function, which is far more explosive than a polynomial.
Of course it will brake itself at some stage, but I would expect to see (if this does get out of hand) a similar curvature occur in the new infections graph, also.
Maybe the fact that the infected die (or recover to become relatively non infectious) somewhat limits the maximum exponentiation.
The point to think about however, is that when plotted on a log normal graph paper, the number of infections looks like a straight line.
Now *that* should give us pause to think about forecasts.
The 20000 number looks like a bit of a forlorn hopefulness - this can get very, very big into the tens or hundreds of thousands, and we'd be lucky if that.
At this rate, counting will become very difficult within a month or two, and all semblance of control in these regions will be lost. I hope I'm wrong and hysterical - but I can't see how they have the staffing to effectively quarantine after one or two more doublings.
Jason (12) My case number line is a polynomial. But it produces the same result reported by epidemiologists using exponential models, at the moment: 10K or more by late December.
The thing is I'm pretty sure the entire analysis is bogus. I think the number of reported cases per day is a function of how many beds there are in the treatment center. A jump in infection rate is actually the addition of a clinic or expansion of a clinic to add beds. The daily infection rate otherwise is simply the number of people who get better or die making room for more in the clinics.
It is possible that your last paragraph already pertains.
The people in the discussion I referenced came back to this several times. To paraphrase their opinion: If that were to occur things would quickly go to shit over a wide region. Not a comforting conclusion.
HIV has been mutating in a large host for a long time.
It had not become airborne. I do suspect that catastrophising about this virus becoming airborne is closer to science fiction.
HPV, HIV, HSV for instance have never mutated to become airborne. It seems like a leap to imagine this would.
I would like to see a virus expert talk about the general patterns of what kind of viruses tend to be fairborn, which kinds, if any, really can't be, etc.
@Greg Laden -- Where did you find those exponential models? (#13) The ones I've read about are predicting 10,000 within *this month*, rather than late December! And over 100,000 in December:
http://news.sciencemag.org/health/2014/08/disease-modelers-project-rapi…
Another model predicts 8,000-55,000 cases through early October -- for some perspective on the uncertainty! The higher estimate is a scenario with a higher exponential constant (R0), because of a breakdown in containing and quarantining ebola patients.
http://cpid.iri.columbia.edu/ebola.html
http://www.nytimes.com/2014/09/13/world/africa/us-scientists-see-long-f…
(I am not an epidemologist)
I was being conservative.
Data on infections and fatalities seems to be more sporatic as the epidemic entensifies. At some point in time (may have been reached) local health services reporting to the WHO will be unable to supply reliable data.
The last three data points don't fit the second chart for cases and deaths. You could double your projections.
Best Guess: WHO is now only supplying regular information by twitter, and sparingly so. the current infection rate is about the same as previously according to that indicating either that the epidemic is waning or they are simply unable to keep track. I think the point you mention was reached a few weeks ago, but hopefully with more resources going in now it will be unreached.