
When it comes to the use of what is sometimes called "complementary and alternative medicine" (CAM) or, increasingly, "integrative medicine," there is a certain narrative. It's a narrative promoted by CAM proponents that does its best to convince the public that there is nothing unusual, untoward, or odd about CAM use, even though much of CAM consists of treatments that are based on prescientific concepts of human physiology and pathology, such as traditional Chinese medicine or homeopathy. In other words, it's a narrative designed to "normalize" CAM usage (and therefore CAM practice), making it no different than the usage of treatments rooted in scientific medicine. And so it isn't, at least, if you're a CAM proponent.
Thus are born studies that spawn press releases like this one entitled Beliefs about complementary and alternative medicine predict use among patients with cancer:
A new study has shed light on how cancer patients' attitudes and beliefs drive the use of complementary and alternative medicine. Published early online in CANCER, a peer-reviewed journal of the American Cancer Society, the findings may help hospitals develop more effective and accessible integrative oncology services for patients.Although many cancer patients use complementary and alternative medicine, what drives this usage is unclear. To investigate, a team led by Jun Mao, MD and Joshua Bauml, MD, of the Abramson Cancer Center at the University of Pennsylvania's Perelman School of Medicine, conducted a survey-based study in their institution's thoracic, breast, and gastrointestinal medical oncology clinics.
The actual study can be found here, entitled Do attitudes and beliefs regarding complementary and alternative medicine impact its use among patients with cancer? A cross-sectional survey. It's a study out of the Abramson Cancer Center at the University of Pennsylvania, and it's a great example of studies designed to support the "normalization" of CAM treatments. Basically, it's a glorified survey that concludes—brace yourself—that people use CAM if the expect benefit and the barriers to using it are not too great and that attitudes and beliefs towards CAM explain much more of the variance in CAM usage than clinical or demographic variables alone.
Or, as Dr. Mao is reported saying in the press release:
"We found that specific attitudes and beliefs -- such as expectation of therapeutic benefits, patient-perceived barriers regarding cost and access, and opinions of patients' physician and family members -- may predict patients' use of complementary and alternative medicine following cancer diagnoses," said Dr. Mao. "We also found that these beliefs and attitudes varied by key socio-demographic factors such as sex, race, and education, which highlights the need for a more individualized approach when clinically integrating complementary and alternative medicine into conventional cancer care."
Well, duh. I doubt anyone would use CAM (or any other medical intervention, be it science-based or, as in the case of CAM, pseudoscience-based) if he didn't expect to benefit from it. That's why people come to doctors. They want and expect to be made better, or at least to have their symptoms improved. That's what medicine is for. It's what we do, or at least try to do, as health care providers. They don't expect to have no result or to get worse. The problem is not the motivation; the problem is that CAM or "integrative medicine" largely sells patients a bill of goods, goods patients are willing to buy given that there are Very Serious People in White Coats telling them that it's all scientific.
To be fair, there were other findings in the survey, which was administered to 969 participants (for a response rate of 83%) that included patients with breast, lung, and gastrointestinal cancers. They used an instrument called Attitudes and Beliefs about CAM, or ABCAM (is that anything like Abacab?), which was developed by the same group and designed to evaluate specific behavioral predictors of CAM use based on the Theory of Planned Behavior. They also looked at CAM use since the cancer diagnosis. Interestingly, the authors intentionally left out spirituality and religion, which are often lumped together with CAM in order to make it seem as though far more people use CAM than actually do. After all, religiosity predominates in the US, at least, and if you can view praying to get well or other spiritual activities as somehow being CAM, then, yes, the vast majority of the population does appear to use CAM, particularly if you also co-opt science-based lifestyle interventions (such as exercise and diet) as also being CAM. It's the appeal to popularity that CAM advocates love to use so much. Indeed, the authors use it right in the beginning of the article:
Cancer accounts for nearly 1 of every 4 deaths occurring in the United States, but recent advances in therapeutics have led to improved survival after diagnosis. As of January 1, 2012, there were approximately 13.7 million cancer survivors living in the United States, and this patient population is growing.2 To meet their unique needs, patients with cancer seek treatments both within and outside the standard allopathic paradigm. Indeed, up to 67% of cancer survivors use complementary and alternative medicine (CAM). Most CAM modalities are based on centuries-old traditions and have historically not been supported by modern evidence. However, more recently, there have been studies demonstrating efficacy for selected therapies in the treatment of multiple cancer-related toxicities.6-8 The evidence-based incorporation of these modalities into traditional cancer care is an emerging field, and is termed integrative oncology.9 Many leading academic cancer centers are developing integrative oncology centers to ensure that the research concerning CAM efficacy is performed in a scientifically rigorous fashion.
Note the appeal to antiquity ("based on centuries-old traditions") and the CAM-speak (the "evidence-based incorporation of these modalities into traditional cancer care"). Particularly annoying is the claim that "integrative medicine" programs exist to "ensure that the research concerning CAM efficacy is performed in a scientifically rigorous fashion." Long time readers will recall the numerous examples over the last decade where I showed that CAM research is, by and large, hardly "rigorous." Indeed, when I discussed the strategic plan of the National Center for Complementary and Integrative Health (NCCIH, the government agency formerly known as the National Center for Complementary and Alternative Medicine, or the easier acronym NCCAM), I referred to it as basically saying "let's do some real science for a change."
In any case, what the authors also report the following.
- Female sex and college education are associated with a significantly higher expectation of benefit from CAM. (I wonder if this at least partially explains phenomenon such as the wine-loving, autism biomed aficionados known as the "Thinking Moms' Revolution," many of whom are college-educated.)
- Nonwhite patients reported more perceived barriers to CAM use compared with white patients but had a similar degree of expected benefit. (Another "Well, duh!" finding. Nonwhite patients in general encounter more perceived barriers to using real medicine than whites; it's no surprise that they would perceive more barriers to CAM usage than whites.)
- Attitudes and beliefs regarding CAM explained much more variance in CAM use than clinical and demographic variables alone.
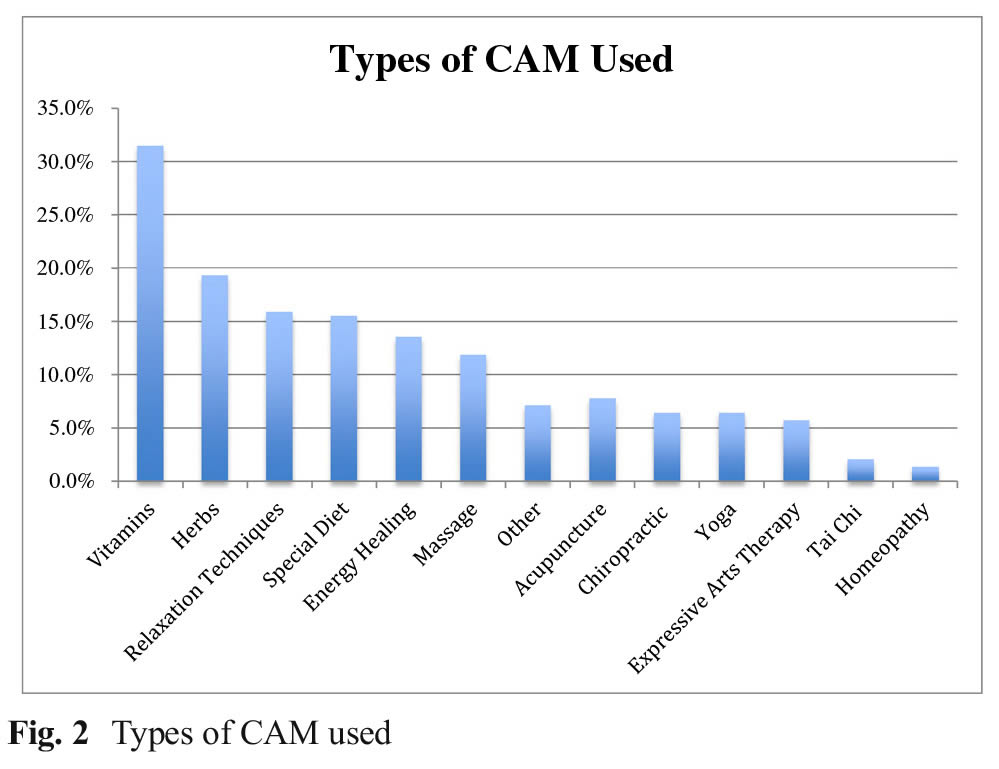
Interestingly, the authors also referenced a previous study of theirs which looked at what kinds of CAM their cancer patients used, in this case lung cancer:
 CAM use in cancer
CAM use in cancer
Not surprisingly, vitamins, herbs, relaxation techniques, and diet were the top four. I was a little surprised that energy healing ranked so high, given that, of all the forms of "integrative medicine" or CAM, "energy healing" (e.g., therapeutic touch or reiki) is definitely one of the quackiest, if not the quackiest, but then I remembered how reiki programs have been springing up like so much kudzu all over even in NCI-designated comprehensive cancer centers. Then there's massage, yoga, and the like, with homeopathy (the other quackiest of CAM modalities, along with reiki) bringing up the rear.
That oddity aside, one thing you have to remember is this: Studies like this are done for a purpose. For instance, when they are done for various conventional medicine modalities, it's called health disparities research, which, as its name suggests, is designed to identify and remedy disparities in disease prevalence and health care based on race, socioeconomic status, gender, and the like. The idea in this particular variety of health disparities research is to identify various beliefs about treatment and perceived barriers to receiving it with the intent of developing and testing strategies to overcome them and eliminate the disparities identified. It's an important area of medical research, given that there are often huge disparities in care based on socioeconomic factors and race, as I know all too well practicing at the cancer center that I practice at.
This is why I refer to research such as this as either evidence of or an effort to "normalize" CAM. If CAM is viewed as just another medical treatment in "conventional medicine," then of course it's only natural that researchers would want to study disparities in CAM care just like any other medical care. Indeed, the authors explicitly say as much, with this unwritten assumption underlying their conclusions:
In viewing CAM use as a health behavior that aims to improve specific cancer-related toxicities, we can potentially target attitudes and beliefs to develop patientcentered integration of CAM into usual cancer care. This would lead to broader access to CAM, and allow for further research into the efficacy of these treatment modalities. For example, patients with lung cancer have a high symptom burden compared with patients with other malignancies, but based purely on demographic factors classically associated with CAM use (eg, female sex and lack of a tobacco history), they may not be targeted for CAM interventions. However, our group has previously shown that CAM use among patients with lung cancer is comparable to that noted in population studies. The current study indicates that attitudes and beliefs regarding CAM may be an important force driving this discrepancy. By targeting integrative oncology programs based on attitudes and beliefs, we will be able to evaluate efficacy in the broadest population possible.
And:
Its limitations notwithstanding, the current study has several important implications. Although population studies have established clinical and demographic factors associated with CAM use, such analyses have limited ability to characterize why patients with cancer use CAM. For example, clinical and demographic factors fail to identify patients who are interested in CAM but who do not use services due to perceived barriers. The social demographic variations in attitudes and beliefs identified in the current study may serve as a foundation for the development of theory-driven interventions that can target the beliefs and attitudes that ultimately influence the use of CAM among patients with cancer. A better understanding of the psychological components of CAM use is essential to delivering comprehensive, patient-centered care. By targeting new integrative oncology programs based on attitudes and beliefs, rather than on clinical and demographic factors or existing use, we may be able to broaden access to these treatments.
Of course, the assumption underlying this study is that CAM use is a good thing that relieves cancer-related symptoms, when most of it is, as I frequently point out, pseudoscientific rubbish mixed with science-based modalities like diet and exercise, which have been "rebranded" somehow as being "alternative" or "integrative." If you buy into that assumption, then of course disparities in CAM use are a bad thing that need to be eliminated (or at least minimized), so that all might have access to the wonders of CAM. Basically, this study, which is a perfectly fine study as far as health disparity studies go, is simply more evidence of how deeply embedded quackademic medicine has become in medical academia. It's to the point where not only are major medical universities studying pseudoscientific treatments like energy healing and acupuncture but they're trying to find out ways to eliminate "disparities" in access and usage to these treatments, just as though they were legitimate science-based medicine.
That profoundly depresses me.
Oh, crikies. These people are both MDs and they use the term "allopathic"? Ugh.
I wonder about this: Could you get hold of the raw data to see what other surprises they might hold?
For example what if it turns out that there are racial as well as gender factors related to belief in sCAM as compared to belief in SBM? At that point we might look for indications that sCAM is being touted to minority communities as having 'fewer barriers to access' as compared to SBM. You know where this is going: the high probability of sCAMmers cashing in on the suffering and death of minority patients.
Yes, I'm advocating going fishing for correlations, but any found correlation can subsequently be tested: and one could make the case that it's incumbent upon the promoters of this study to do so, precisely in order to prevent a pack of sCAMmers swooping down on one or another unsuspecting community.
---
I see that word 'toxicity' again: 'However, more recently, there have been studies demonstrating efficacy for selected therapies in the treatment of multiple cancer-related toxicities.' Is that 'toxicity' as in SBM-recognised effects, or is that our old nemesis, 'Toxicity' with a capital T as in 'quick, put some coffee up your bum!'...?
---
The good news is that homeoquackery does indeed 'bring up the rear,' with about 2% of patients resorting to magic water. That would be a number worth following over time to see if it decreases.
Could be worse. They could have used it correctly.
The word "allopathic," that is.
My translation: We are going to find the group of patients that want CAM but can’t afford it, then make our appeal to have energy healing and acupuncture covered by Medicare/Medicaid.
If one starts from the position that sCAM is effective, it is only a small step to see it as a social justice issue. The poor! The toxicities! Freedom for all who believe!
Very nice that they are so open about using this as a means of making quite a bit of money.....
Interesting -- there are a half-dozen things on that list that I don't necessarily consider CAM, things like vitamins, massage, yoga, Tai Chi, relaxation techniques, expressive art therapy, and (maybe) diet.
@ lynn
I was actually disappointed to find various meditation/exercise modalities near the far end of the list. I would have hoped for yoga and tai-chi to have more amateurs than energy healing.
Lynn @ 7:
Many of these things are perfectly OK for exercise and emotional benefits and so on. Many of them increase happiness and quality of life. But the problem we, here, have with them is when they are touted by quacks as producing specific medical benefits that are not supported by peer-reviewed research.
Massage, relaxation, art therapy, etc., produce good feelings. Yoga and Tai Chi are perfectly good forms of exercise, especially for people who are engaged with Asian-tradition beliefs (and we shouldn't insist on patients only getting 'atheistic exercise' whatever that might be:-). Good feelings are good by definition. Happiness is good, relaxation is good, etc. etc. But happiness and good feelings are not substitutes for medical treatments that are strongly supported by rigourous research.
The deeper underlying problem is that Anglo/American cultures are still suffering from the disease of Puritanism (and in America, neo-Calvinism). One of the primary symptoms is the disapproval of other people having any form of pleasure, particularly bodily pleasure. Another is the (IMHO delusional) belief that suffering is somehow deserved. Thus we see various abuses such as making chronic pain patients suffer needlessly in order to 'protect' them from 'addiction' to narcotic analgesics. Bloody hell!, if you're fully disabled or facing death at close range, whose business is it if you become dependent on morphine?
That climate creates an incentive for humane and compassionate physicians to seek ways to get quality-of-life interventions approved as part of medical regimens. So far so good, we want quality-of-live interventions approved! Everyone with a microgramme of empathy wants cancer patients etc. to feel happier while they're getting their chemo and surgery to fight the disease!
However, that in turn creates a climate where cynical quacks and misguided True Believers can jump on the band wagon, and seek to make large amounts of money or promote their philosophies of life, by peddling their wares as actual treatments for disease. This happens to a very large degree, with horrible outcomes for patients. And that gets us to where we are now, with Orac having to tear this stuff to shreds, lest it keep patients from getting the real medical treatments that may save or extend their lives.
Lurker writes (#9) writes: But the problem we, here, have with them is when they are touted by quacks as producing specific medical benefits that are not supported by peer-reviewed research.
Of course. It seems to me, however, that lumping them in willy-nilly with CAM serves to obfuscate the issues. I can well imagine someone saying, "Well, they think yoga is CAM and I know it's good for flexibility and balance, so maybe they're wrong about the other things, too."
The 'bad guys' are claiming all these things are good, when that's not accurate. We're claiming they're all bad, yet tht's not accurate either.
Correction -- we seem to be claiming they're all bad.
@ Lynn
"We seem", indeed.
Because nutrition, yoga, etc are not perceived as medical acts in themselves (medicine is just about "cut and poison", isn't it - surgery and drugs); because some alt-med con-men are very smart, and because doing exercise, etc is an active choice while landing in an hospital bed is something we usually don't have much control over, these modalities have been hijacked by CAM practionners.
Imagine no more. That's precisely the reason why nutrition and relaxation are trotted along supplements.
A couple of things...
- " the incorporation of these modalities into traditional cancer care"
I've noticed that some alties use TRADITIONAL to refer to SBM or EBM as if to suggest that CAM/ IM is the new wave/ next paradigm although they may also refer to TCM or Ayurveda as traditional, appealing to antiquity.
I wish they'd make up their minds.
- re non-whites' perception of barriers to accessing CAM/IM.
Right and woo-meisters like Null are on-task here by specifically appealing to ethnic lifestyle differences and possible political issues .
If you look at 'health retreat' photos ( @ Gary Null.com), you'll observe that the number on non-white participants is much larger than would be expected by chance based upon subjects' most likely domestic location.
Mikey balances his occasional political incorrectness with equally insensitive pandering to nonwhites.
-
"Atheistic exercise"?
That'll be what I did earlier today when I went out for a 7-8 mile walk: 's exercise and I'm an atheist...
And it'll be the same tomorrow, weather permitting...
Helianthus (12) Imagine no more. That’s precisely the reason why nutrition and relaxation are trotted along supplements."
So how do we reclaim these things for real medicine?
When I talk with people about "evil western medicine," I note the last 3 prescriptions my MDs have given me:
buy a pedometer (borderline hypertension)
physical therapy/weight lifting (osteoarthritis)
2-3 specific yoga positions (improved back flexibility)
The reaction? "Cool! Your MD is into alternative medicine."
Well, yes. That's part of the point. A lot of perfectly valid lifestyle interventions have been co-opted as being somehow "alternative" or "integrative" when they are part of conventional medicine. (I'm counting Tai Chi and yoga as forms of exercise.) Either that, or various modalities that we used to view as supportive care (art, music, massage) have also been co-opted, even though we used to view such activities as things that either help patients pass the time in the hospital or help them feel less depressed at home. Indeed, I've referred to these modalities as having been "medicalized" by CAM. By co-opting such modalities and lumping them together with the more woo-ey CAM, proponents give the impression of efficacy and harmlessness by association to the quackery.
This is the concept of the "Trojan horse." You wrap the hard core quackery, like homeopathy, reiki, much of traditional Chinese medicine, etc. in the normal-appearing "horse" of modalities like these, and that's how CAM and integrative medicine sneak into the fortresses of medical academia. Once the exercise, diet, etc. are inside the walls, the hard core woo jumps out to take over. Academic medicine becomes quackademic medicine.
OK, it's not a perfect analogy, but I think you get the idea.
@ Lynn
Frankly? Tell these people they are !diots. You cannot stop believers from believing.
@ Helianthus "Frankly? Tell these people they are !diots. You cannot stop believers from believing."
I pretty much do.
But there still should be some way to reclaim some of those things for real medicine.
Atheistic exercise is all well and good, until you're 20 miles into a marathon. Then it's "Oh God, I can't go on..."
@Orac #16:
Perfect analogy or not, we need more Laocoons throwing spears. We just need to employ snake charmers too ;-)
"Once the exercise, diet, etc. are inside the walls, the hard core woo jumps out to take over"
But how did they get outside the walls? And, as I keep asking, how do we reclaim them?
When the authors of the article talk about "targeting attitudes and belief", do they mean "finding people who want CAM but haven't asked" or do they mean "change patients' thoughts about CAM so that they ask for it"?
Because the first thing is sort of obnoxious, but expected. The second thing is nasty and skirts awfully close to unethical. If I'm already sick the last thing I want is some quack trying to wear me down into accepting their quacky treatment.
Lynn - we might be out of luck for yoga and tai chi. They have been pretty thoroughly taken over by the woos as their own. Unfortunately it is often difficult to find a good yoga class where the instructor is not a hard core woo. I had a great instructor at one point, but after that a series of disappointments. It doesn't help that the woos also claim superior knowledge of diet and lifestyle interventions. Part of the problem there is the fact that the large group of 'shruggie' physicians are not actively combating this. I have gotten lifestyle advice at every doctor's visit forever, but you find few docs wading to say what they do for their patients. As long as the woos continue to paint MDs with the broad brush of pill poppers only interested in drugs and surgery and the docs don't step up and defend themselves then they are going to lost the fight.
@ Lynn
My apologies for the previous answer, it was a bit too snappy. I sometimes get fed up with all this antiscience BS.
The outside the wall part, I'm afraid, is just the normal course of life. Things get in and out of fashion. A few decades ago, fictions were full of people commenting on their physician advising them to do more sport or to cut on the calories. Then physicians become the guys you meet for a medical emergency. Now, physicians are drug addicts with the bedside manner of a bulldog with impacted teeth. Fables and fashions are cyclic events, so maybe the all-wise physician will come back.
Concepts get eroded through their passage from one subculture to the next, lose part of their meaning, or at least become more fuzzy. We became blasé about medicine, science and their actors.
Sysiphe get tired of pushing his rock uphill and just let it roll down. Physicians give up on telling people to stop worrying and prescribe them something to get rid of them.
(A few buddies of Orac adopted Sysiphe as a symbol of their dedication for promoting science-based medicine, I'm suddenly very aware how apropos it is).
We French tend to stereotype Americans as people looking for a pill to cure whatever ails them. I'm afraid it may have some grain of truth, and it may be an attitude shared in all societies. We want simple answers.
In short, for better and for worse, we see doctors as pill-pushers. Exercise, learn yoga, take lessons in art? Heck, these are all hobbies. I didn't give 20 bucks to the doc to be counseled on how to spent my evenings, I want a medicine.
(an old satyrical French theater play/movie, Dr Knock, has a scene on similar lines)
So we are primed to recognize as a healer anyone ready to hand us pills and a promise of better health.
And, flip side of the coin, anything outside of little pills will be considered as not-medicine. So you don't go to your physician for nutrition or exercise advice, what does he/she know?
The hard part, how to reclaim them?
Keep correcting people. Be the voice of common sense. Talk about your personal experiences, how they contradict their assumptions.
Make no mistake, it will be a Sisyphean task.
And the most difficult, learn not to argue in the face of idiocy.
And don't feed the smarter-than-you trolls. Those are beyond anyone's reach.
(both last cases I'm a utter failure at)
It will also help if physicians can spend more than 5 minutes talking with their patients.
@Lynn
I wouldn't consider vitamins/supplements part of medicine, unless prescribed by an MD for a lab confirmed (normal lab, not spit and such) deficiency. I think it might even be that vitamins are a "gateway drug" to CAM.
Vitamins/supplements can be a slightly fuzzy spectrum (no pun intended). At one end you have a prescribed vitamin, mineral or other supplement to compensate for a known, tested deficiency. At the other end you have "magic enhancement herbs" made by some dude in a warehouse.
And in the middle you have things like when my doctor said "Look, you're a pasty white girl in a city that gets very little sunlight, and you've said you might consider children in the future. Take a calcium/vitamin D supplement, as written on the label." That seems like good common sense, backed up with data.
And I think it's things like that, just like the yoga, walking and physical therapy that are perfectly normal and sound, but get co-opted by the CAM. How many of the 31% of people who reported "using vitamins" were talking about calcium, or vitamin C throat drops, versus 100X RDA vitamin D?
Speaking of disparities, the Dachelbot seems to be enraged that Israeli haredi families don't much care about what she does:
"Fears that vaccines are linked to autism - such connections have been debunked by the scientific research - are cited less frequently in Israel than they are in the United States.
"Most of the story is about welfare in Israel.[*] Reporter Ben Sales could care less if vaccines carry any risks. Above is the ONE SENTENCE ON THE SUBJECT."
* Oddly, it is a story about child subsidies in Israel.
@#5 CTGeneGuy
My son is disabled due to severe congenital heart issues and mild learning issues, As I type, I have on my desk his CMO/managed care selection flyer for his shiny new Medicaid.
One of the plans offers 25% discount on: Acupuncture, Chiropractic, and Massage Therapy (I would go for that last, feels so good)
Another offers "Acupuncture for substance abuse treatment"
So, too late....
[sigh]
I guess I shouldn’t be surprised, Blues.
I would be interested to see a discussion of the economics of this. Managed care groups do their homework, so there must be a reason why they would offer these benefits that they don’t have to offer. Is it to attract and compete for enrollees in the new healthcare marketplaces? Have they determined that people who seek such benefits are “good” customers in the sense that they are a relatively healthy subpopulation (“targeting” the worried well alt med crowd)?